 Back
BackThe Urinary System: Structure, Function, and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Urinary System
Overview and Functions
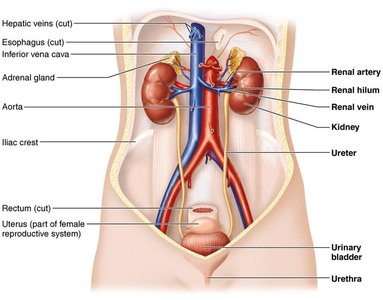
The urinary system is essential for maintaining the body's internal environment by regulating water, solute concentrations, and removing metabolic wastes. It consists of the kidneys, ureters, urinary bladder, and urethra.
Regulation of water and solute balance: Kidneys adjust total water volume and solute concentration in the body.
Ion regulation: Control of ion concentrations in extracellular fluid (ECF).
Acid-base balance: Ensures long-term acid-base equilibrium.
Excretion: Removal of metabolic wastes, toxins, and drugs.
Hormone production: Erythropoietin (stimulates RBC production) and renin (regulates blood pressure).
Vitamin D activation and gluconeogenesis (if needed).
Anatomy of the Kidneys
Gross Structure
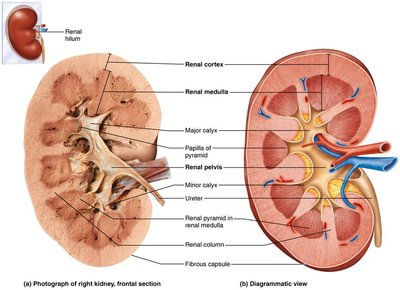
The kidneys are retroperitoneal organs with a complex internal structure designed for filtration and urine formation.
Renal cortex: Outer region containing most nephrons.
Renal medulla: Inner region with renal pyramids.
Renal pelvis: Funnel-shaped tube that collects urine and channels it to the ureter.
Major and minor calyces: Collect urine from papillae of pyramids.
Blood Supply
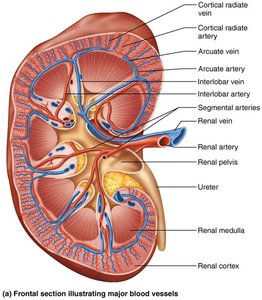
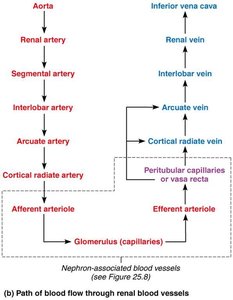
The kidneys receive a rich blood supply, essential for filtration and homeostasis. Blood flows through a series of arteries and veins, eventually reaching the nephrons for filtration.
Renal artery → Segmental artery → Interlobar artery → Arcuate artery → Cortical radiate artery → Afferent arteriole → Glomerulus → Efferent arteriole → Peritubular capillaries/vasa recta → Cortical radiate vein → Arcuate vein → Interlobar vein → Renal vein
Nephrons: The Functional Units
Structure of Nephrons
Nephrons are the microscopic structural and functional units of the kidney, responsible for urine formation. Each kidney contains over one million nephrons.
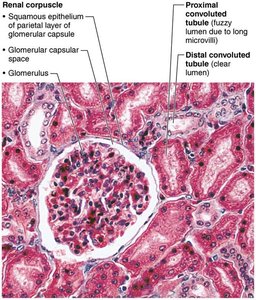
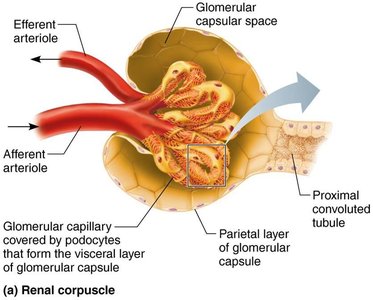
Renal corpuscle: Includes the glomerulus (a tuft of capillaries) and the glomerular (Bowman's) capsule.
Renal tubule: Composed of the proximal convoluted tubule (PCT), nephron loop (loop of Henle), and distal convoluted tubule (DCT).
Collecting duct: Receives filtrate from multiple nephrons and participates in final urine concentration.
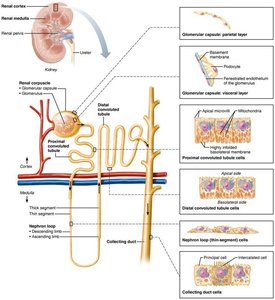
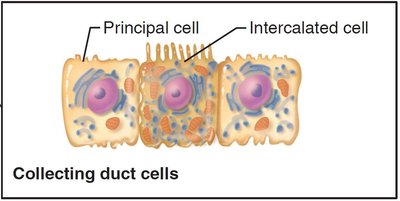
Cell Types in the Collecting Duct
Principal cells: Regulate water and sodium balance.
Intercalated cells (Type A and B): Regulate acid-base balance.
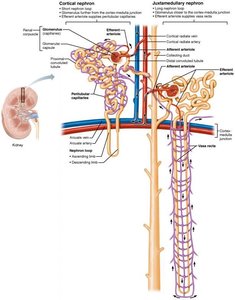
Types of Nephrons
Cortical nephrons: 85% of nephrons, located mostly in the cortex, associated with peritubular capillaries.
Juxtamedullary nephrons: Long nephron loops extend deep into the medulla, associated with vasa recta, crucial for producing concentrated urine.
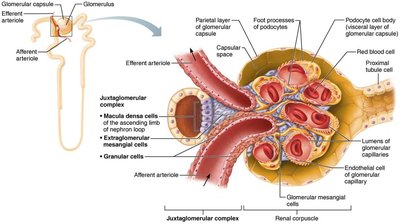
Juxtaglomerular Complex (JGC)
The JGC is a specialized structure that regulates filtrate formation and blood pressure.
Macula densa: Chemoreceptors that sense NaCl content in filtrate.
Granular (JG) cells: Mechanoreceptors that sense blood pressure and secrete renin.
Extraglomerular mesangial cells: May relay signals between macula densa and granular cells.
Physiology of the Kidney
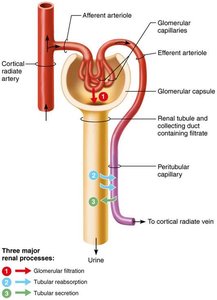
Urine Formation
The kidneys process about 180 L of fluid daily, but only 1.5 L of urine is excreted. Urine formation involves three main processes:
Glomerular filtration: Passive process producing cell- and protein-free filtrate.
Tubular reabsorption: Selective return of 99% of substances from filtrate to blood.
Tubular secretion: Selective movement of substances from blood to filtrate.
Glomerular Filtration
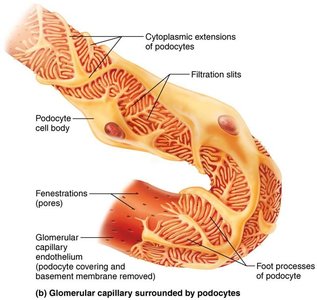
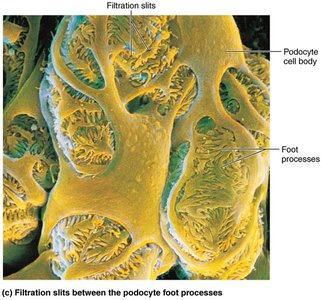
Filtration occurs across a porous membrane between the blood and the glomerular capsule. Hydrostatic pressure forces water and solutes through, but cells and most proteins are retained in the blood.
Filtration membrane: Consists of fenestrated endothelium, basement membrane, and podocyte foot processes with filtration slits.
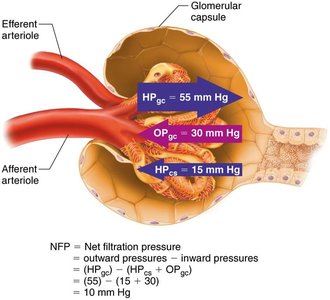
Net Filtration Pressure (NFP)
NFP is the balance of pressures driving filtration at the glomerulus:
Glomerular hydrostatic pressure (HPgc): Outward pressure (55 mm Hg).
Colloid osmotic pressure (OPgc): Inward pressure (30 mm Hg).
Capsular hydrostatic pressure (HPcs): Inward pressure (15 mm Hg).
Equation:
Glomerular Filtration Rate (GFR)
GFR is the volume of filtrate formed per minute by both kidneys (normal: 120–125 ml/min). It is directly proportional to:
Net filtration pressure (NFP)
Total surface area available for filtration
Filtration membrane permeability
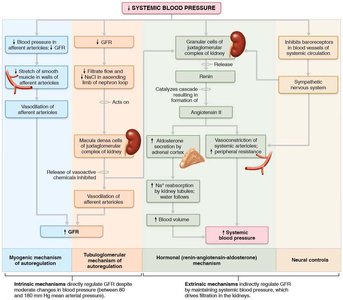
Regulation of GFR
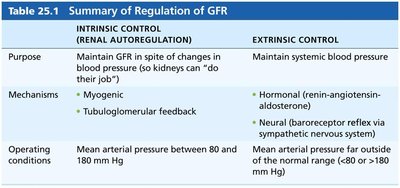
GFR must be tightly regulated to maintain homeostasis and systemic blood pressure. Regulation involves intrinsic (renal autoregulation) and extrinsic (neural and hormonal) controls.
Intrinsic controls: Myogenic mechanism and tubuloglomerular feedback maintain GFR when mean arterial pressure is 80–180 mm Hg.
Extrinsic controls: Sympathetic nervous system and renin-angiotensin-aldosterone system maintain systemic blood pressure.
Intrinsic Control (Renal Autoregulation) | Extrinsic Control |
|---|---|
Maintain GFR in spite of changes in blood pressure | Maintain systemic blood pressure |
Myogenic, Tubuloglomerular feedback | Hormonal (renin-angiotensin-aldosterone), Neural (baroreceptor reflex) |
MAP 80–180 mm Hg | MAP outside 80–180 mm Hg |
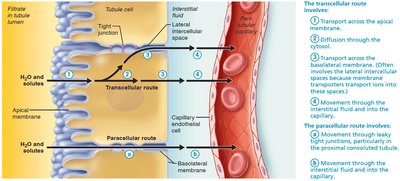
Tubular Reabsorption
Mechanisms and Routes
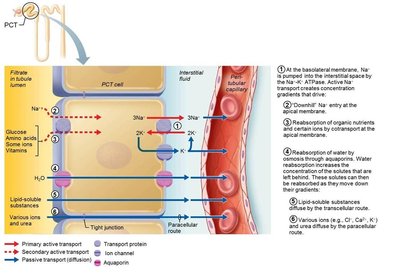
Tubular reabsorption reclaims most filtrate components back into the blood via transcellular (through cells) and paracellular (between cells) routes. It involves both active and passive transport mechanisms.
Transport Maximum (Tm)
Each solute has a transport maximum, reflecting the number of available carriers. When exceeded, excess solute is excreted in urine (e.g., glucose in diabetes mellitus).
Segmental Reabsorptive Capabilities
Proximal convoluted tubule (PCT): Site of most reabsorption (all nutrients, 65% Na+ and water, many ions).
Nephron loop: Descending limb reabsorbs water; ascending limb reabsorbs solutes (Na+, Cl−).
Distal convoluted tubule (DCT) and collecting duct: Reabsorption is hormonally regulated (ADH, aldosterone, atrial natriuretic peptide, parathyroid hormone).
Tubular Secretion
Purpose and Mechanisms
Tubular secretion is the movement of substances from blood into the filtrate, primarily in the PCT. It is essential for:
Eliminating drugs, metabolites, and excess K+
Controlling blood pH by secreting H+ or HCO3−
Removing substances passively reabsorbed (e.g., urea, uric acid)
Regulation of Urine Concentration and Volume
Countercurrent Mechanism
The kidneys use a countercurrent mechanism (fluid flows in opposite directions in adjacent segments of the nephron loop and vasa recta) to produce concentrated or dilute urine as needed.
Countercurrent multiplier: Nephron loop creates an osmotic gradient in the medulla.
Countercurrent exchanger: Vasa recta preserves the gradient while reabsorbing water and solutes.
Urea recycling: Urea contributes to the medullary osmotic gradient.
Hormonal Regulation
Antidiuretic hormone (ADH): Increases water reabsorption in collecting ducts by inserting aquaporins.
Aldosterone: Increases Na+ reabsorption (and water follows), decreases K+ levels.
Atrial natriuretic peptide (ANP): Reduces Na+ and water reabsorption, lowering blood volume and pressure.
Parathyroid hormone (PTH): Increases Ca2+ reabsorption in DCT.
Diuretics
ADH inhibitors: Alcohol
Na+ reabsorption inhibitors: Caffeine, some drugs
Loop diuretics: Inhibit medullary gradient formation
Osmotic diuretics: Substances not reabsorbed, e.g., glucose in diabetes
Clinical Evaluation of Kidney Function
Urinalysis and Renal Clearance
Urinalysis: Examines urine for disease or illegal substances.
Renal clearance: Volume of plasma cleared of a substance per unit time; used to assess GFR and kidney health.
Urine Composition
95% water, 5% solutes (urea, uric acid, creatinine, ions)
Abnormal components (e.g., blood, proteins, WBCs) may indicate pathology
Transport, Storage, and Elimination of Urine
Ureters
Slender tubes conveying urine from kidneys to bladder
Three layers: mucosa (transitional epithelium), muscularis (smooth muscle), adventitia (connective tissue)
Peristalsis propels urine; backflow is prevented by closure at bladder entry
Urinary Bladder
Muscular sac for temporary urine storage
Layers: mucosa (transitional epithelium), detrusor muscle (three smooth muscle layers), adventitia
Trigone: triangular area prone to infection
Urethra
Muscular tube draining the bladder
Internal urethral sphincter (involuntary, smooth muscle)
External urethral sphincter (voluntary, skeletal muscle)
Male urethra: prostatic, membranous, and spongy regions; carries semen and urine
Female urethra: shorter, only carries urine
Micturition (Urination)
Requires contraction of detrusor (ANS), opening of internal sphincter (ANS), and opening of external sphincter (somatic NS)
Reflexive in infants; voluntary control develops with age
Clinical Considerations
Renal calculi (kidney stones): Crystallized salts can block ureters, causing pain; risk factors include dehydration and high calcium.
Urinary tract infections (UTIs): More common in women; can involve urethra (urethritis), bladder (cystitis), or kidneys (pyelonephritis).
Urinary incontinence: Inability to control urination, often due to weakened pelvic muscles.
