 Back
BackThe Urinary System: Structure, Function, and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Urinary System
Overview of Urinary System Structures
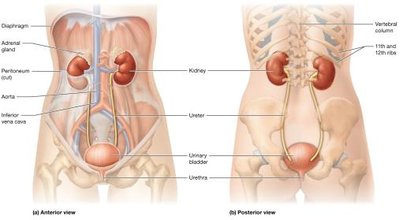
The urinary system is essential for filtering blood, removing metabolic wastes, and maintaining homeostasis of fluids, electrolytes, and acid-base balance. It consists of the paired kidneys and the urinary tract, which includes the ureters, urinary bladder, and urethra.
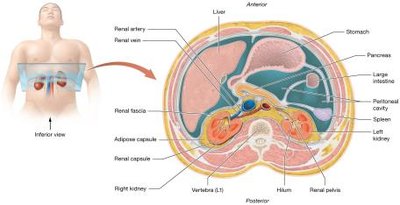
Kidneys: Retroperitoneal organs located against the posterior abdominal wall, partially protected by the 11th and 12th ribs, and capped by adrenal glands.
Urinary Tract: Composed of paired ureters (transport urine from kidneys to bladder), the urinary bladder (stores urine), and the urethra (expels urine from the body).
Functions of the Kidneys
Removal of Metabolic Wastes: Kidneys filter wastes from the blood, including urea, creatinine, and uric acid.
Fluid and Electrolyte Balance: Regulate osmolarity by conserving or eliminating water and electrolytes (e.g., sodium, potassium, calcium).
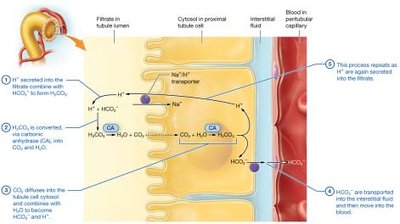
Acid-Base Balance: Maintain blood pH by controlling excretion of hydrogen and bicarbonate ions.
Blood Pressure Regulation: Influence systemic blood pressure via blood volume control and secretion of renin.
Regulation of Erythropoiesis: Release erythropoietin to stimulate red blood cell production.
Other Metabolic Functions: Detoxification, activation of vitamin D, and gluconeogenesis.
Kidney Anatomy
External Anatomy of the Kidneys
Each kidney is surrounded by three layers of connective tissue:
Renal Fascia: Anchors kidney to peritoneum and posterior abdominal wall.
Adipose Capsule: Cushions and protects the kidney; loss can lead to nephroptosis (kidney droop).
Renal Capsule: Thin, dense irregular connective tissue layer protecting from infection and trauma.
The kidney is about 11 cm long, 6 cm wide, and 3 cm thick, weighing about 150 grams. The hilum is the entry/exit site for vessels, nerves, and ureter. The renal sinus is a central cavity containing urine-draining structures and adipose tissue.
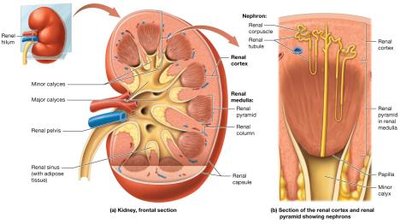
Internal Anatomy of the Kidneys
The kidney is divided into three main regions:
Renal Cortex: Outer region, rich in blood supply, contains most blood vessels and renal columns.
Renal Medulla: Middle region, contains renal (medullary) pyramids separated by renal columns.
Renal Pelvis: Inner collecting chamber for urine, formed by merging major calyces.
Each kidney contains over one million nephrons, the functional units responsible for filtering blood and forming urine.
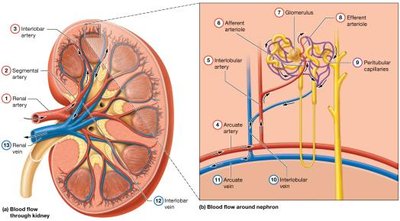
Blood Supply of the Kidneys
The kidneys receive about 25% of cardiac output (1,200 ml/min). Blood flows through a series of arteries and arterioles before reaching the glomerulus, and then exits via veins.
Arterial Pathway: Renal artery → Segmental artery → Interlobar artery → Arcuate artery → Interlobular (cortical radiate) artery → Afferent arteriole → Glomerulus → Efferent arteriole → Peritubular capillaries
Venous Pathway: Interlobular vein → Arcuate vein → Interlobar vein → Renal vein
Microanatomy: The Nephron and Collecting System
Nephron Structure
Each nephron consists of a renal corpuscle (glomerulus and glomerular capsule) and a renal tubule (proximal tubule, nephron loop, distal tubule). The collecting system further modifies filtrate and transports urine.
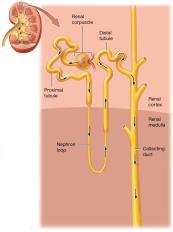
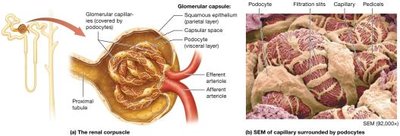
Renal Corpuscle
Glomerulus: Capillary network with fenestrations (pores) for filtration.
Glomerular (Bowman's) Capsule: Double-layered; outer parietal layer (simple squamous epithelium), inner visceral layer (podocytes with filtration slits).
Capsular Space: Area between layers where filtrate collects.
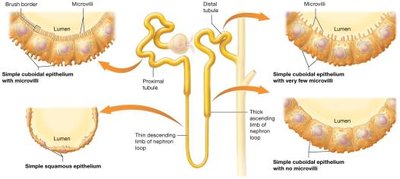
Renal Tubule
Proximal Tubule: Simple cuboidal epithelium with microvilli (brush border) for increased surface area.
Nephron Loop (Loop of Henle): Descending limb (simple squamous), ascending limb (thick, simple cuboidal).
Distal Tubule: Simple cuboidal epithelium, fewer microvilli.
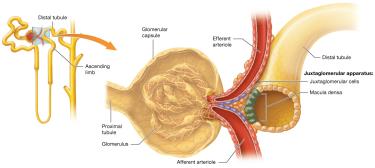
Juxtaglomerular Apparatus (JGA)
Composed of macula densa cells (distal tubule) and juxtaglomerular (JG) cells (afferent/efferent arterioles). Regulates blood pressure and glomerular filtration rate (GFR).
Collecting System
Cortical Collecting Duct: Receives filtrate from distal tubules.
Medullary Collecting Duct: Continues into the renal medulla.
Papillary Ducts: Merge and deliver urine to minor calyces.

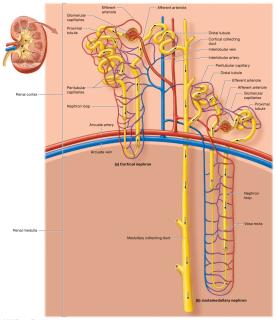
Types of Nephrons
Cortical Nephrons: 80% of nephrons, located in the cortex, short loops.
Juxtamedullary Nephrons: Long loops extend into medulla, surrounded by vasa recta, crucial for urine concentration.
Renal Physiology
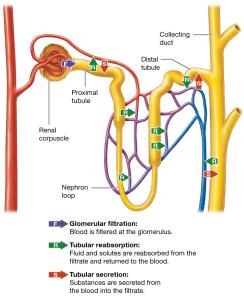
Three Basic Processes
Glomerular Filtration: Blood pressure forces water and solutes from glomerular capillaries into the capsular space, forming filtrate.
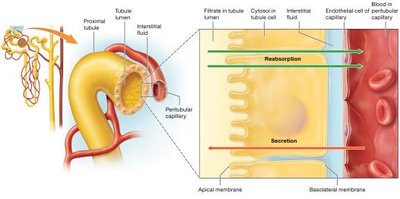
Tubular Reabsorption: Selective movement of substances from filtrate back into blood (mainly in proximal tubule and nephron loop).
Tubular Secretion: Active transport of substances from blood into filtrate for excretion.
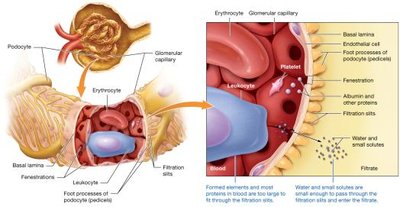
The Filtration Membrane
Fenestrated Endothelial Cells: Allow passage of most solutes but not blood cells or platelets.
Basal Lamina: Meshwork that blocks large and negatively charged proteins.
Podocytes: Form filtration slits, allowing only small molecules (<6–7 nm) to pass.
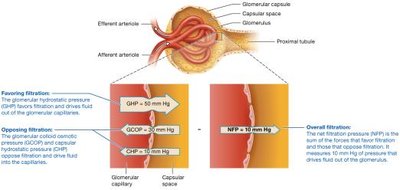
Glomerular Filtration Rate (GFR)
GFR is the rate at which filtrate is formed (about 125 ml/min). It is determined by the net filtration pressure (NFP), which is the balance of hydrostatic and osmotic pressures:
Glomerular Hydrostatic Pressure (GHP): Favors filtration (about 50 mm Hg).
Glomerular Colloid Osmotic Pressure (GCOP): Opposes filtration (about 30 mm Hg).
Capsular Hydrostatic Pressure (CHP): Opposes filtration (about 10 mm Hg).
Net Filtration Pressure (NFP):
Regulation of GFR
Autoregulation
Myogenic Mechanism: Afferent arteriole constricts/dilates in response to blood pressure changes.
Tubuloglomerular Feedback: Macula densa senses NaCl delivery, signals JG cells to adjust arteriole diameter and renin release.
Hormonal Regulation
Renin-Angiotensin-Aldosterone System (RAAS): Activated by low blood pressure, increases GFR by constricting efferent arterioles, increasing Na+ and water reabsorption, and stimulating thirst.
Atrial Natriuretic Peptide (ANP): Released by the heart, increases GFR by dilating afferent and constricting efferent arterioles.
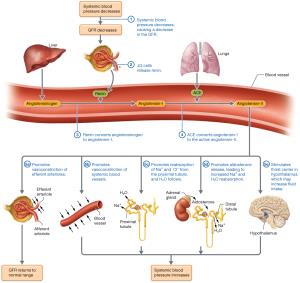
Neural Regulation
Sympathetic nervous system constricts afferent arterioles, reducing GFR during stress or blood loss.
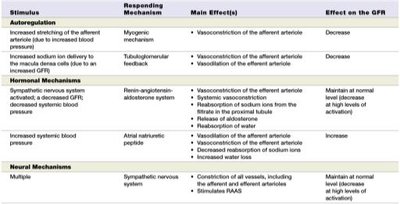
Summary Table: Control of GFR
Stimulus | Responding Mechanism | Main Effect(s) | Effect on GFR |
|---|---|---|---|
Increased afferent arteriole stretch | Myogenic | Vasoconstriction of afferent arteriole | Decrease |
Increased NaCl to macula densa | Tubuloglomerular feedback | Vasoconstriction of afferent arteriole | Decrease |
Low BP/volume | RAAS | Vasoconstriction of efferent arteriole, Na+ reabsorption | Maintain/increase |
Increased blood volume | ANP | Dilation of afferent, constriction of efferent arteriole | Increase |
Sympathetic activation | Neural | Constriction of afferent arteriole | Decrease |
Tubular Reabsorption and Secretion
Principles of Tubular Reabsorption and Secretion
Paracellular Route: Substances pass between tubule cells (e.g., small ions, water).
Transcellular Route: Substances move through tubule cells (e.g., glucose, amino acids).
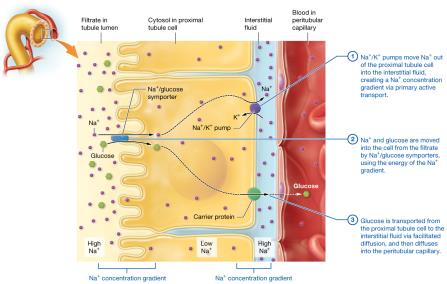
Carrier-Mediated Transport
Facilitated Diffusion: Passive, with concentration gradient.
Primary Active Transport: Uses ATP to move solutes against gradient.
Secondary Active Transport: Uses gradient set up by primary active transport.
Antiporters: Move solutes in opposite directions.
Symporters: Move solutes in the same direction.
Transport Maximum (Tm): Maximum rate of reabsorption; excess solute appears in urine.
Reabsorption and Secretion in the Proximal Tubule
Reabsorbs most electrolytes, nutrients, bicarbonate, and water.
Secretes hydrogen ions, nitrogenous wastes, and drugs.

Reabsorption in the Nephron Loop
Descending Limb: Permeable to water, not solutes; filtrate becomes concentrated.
Ascending Limb: Impermeable to water, actively transports NaCl out; filtrate becomes dilute.
Reabsorption and Secretion in the Distal Tubule and Collecting System
Fine-tunes water, electrolyte, and acid-base balance under hormonal control (aldosterone, ADH, ANP).
Facultative water reabsorption occurs here, depending on body needs.
Urine Concentration and Dilution
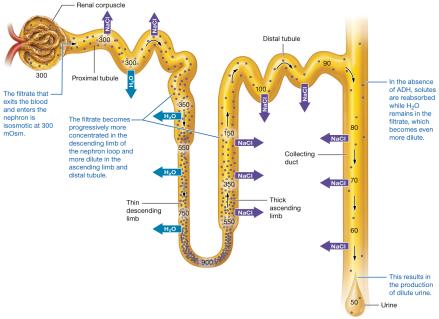
Osmolarity of the Filtrate
Filtrate is isosmotic with plasma in the proximal tubule (~300 mOsm).
Becomes concentrated in the descending limb, diluted in the ascending limb, and further modified in the distal tubule and collecting duct.
Production of Dilute and Concentrated Urine
Dilute Urine: Produced when ADH is low; collecting ducts are impermeable to water.
Concentrated Urine: Produced when ADH is high; water is reabsorbed due to medullary osmotic gradient.
The Countercurrent Mechanism
Countercurrent Multiplier: In juxtamedullary nephrons, establishes medullary osmotic gradient by active transport of NaCl in the ascending limb and water reabsorption in the descending limb.
Urea Recycling: Contributes to medullary osmotic gradient.
Countercurrent Exchanger: Vasa recta maintains the gradient by exchanging water and solutes without dissipating the gradient.
Urine Composition and Urinalysis
Normal Urine Composition
Water, sodium, potassium, chloride, hydrogen ions, phosphates, sulfates, urea, creatinine, ammonia, uric acid, trace bicarbonate, calcium, magnesium.
Urinalysis
Color: Yellow due to urochrome; varies with concentration and diet.
Translucency: Cloudiness may indicate infection or proteinuria.
Odor: Mild when fresh; strong ammonia odor if standing; altered by disease or diet.
pH: Normally ~6.0 (range 4.5–8.0).
Specific Gravity: 1.001–1.035 (higher than water).
Urine Transport, Storage, and Elimination
Urinary Tract Anatomy
Ureters: Transport urine from kidneys to bladder via peristalsis; lined with transitional epithelium.
Urinary Bladder: Stores urine; detrusor muscle contracts during micturition; mucosa protects from urine.
Trigone: Triangular area in bladder floor, bounded by ureteral orifices and internal urethral orifice.
Urethra: Drains urine from bladder to outside; shorter in females, longer and divided into regions in males.
Micturition (Urination)
Micturition Reflex: Initiated by stretch receptors in bladder wall; parasympathetic stimulation contracts detrusor muscle and relaxes internal sphincter.
Voluntary Control: External urethral sphincter (skeletal muscle) allows conscious control; overridden if bladder volume exceeds 500–600 ml.
Clinical Connections
Nephrolithiasis (Kidney Stones): Crystalline stones (often calcium oxalate) form in the urinary tract, causing pain, hematuria, and possible obstruction.
Glomerulonephritis: Inflammation of glomeruli, leading to proteinuria, hematuria, and possible renal failure.
Renal Failure: Acute or chronic loss of kidney function; may require dialysis or transplantation.
SIADH: Excess ADH secretion causes water retention, hyponatremia, and concentrated urine.
Diuretics: Drugs that increase urine output by inhibiting solute reabsorption at various nephron sites.
Key Equations and Concepts
Net Filtration Pressure (NFP):
Glomerular Filtration Rate (GFR): Normal value ~125 ml/min
Transport Maximum (Tm): Maximum rate of solute reabsorption; exceeded in diabetes mellitus (glycosuria).
Summary Table: Control of GFR
Stimulus | Responding Mechanism | Main Effect(s) | Effect on GFR |
|---|---|---|---|
Increased afferent arteriole stretch | Myogenic | Vasoconstriction of afferent arteriole | Decrease |
Increased NaCl to macula densa | Tubuloglomerular feedback | Vasoconstriction of afferent arteriole | Decrease |
Low BP/volume | RAAS | Vasoconstriction of efferent arteriole, Na+ reabsorption | Maintain/increase |
Increased blood volume | ANP | Dilation of afferent, constriction of efferent arteriole | Increase |
Sympathetic activation | Neural | Constriction of afferent arteriole | Decrease |
Additional info: This guide integrates textbook-level explanations, clinical context, and visual aids for comprehensive understanding of the urinary system, suitable for ANP college students.
