 Back
BackTubular Reabsorption and Secretion: Mechanisms and Regulation in the Urinary System
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tubular Reabsorption
Overview of Tubular Reabsorption
Tubular reabsorption is a critical process in the nephron where most of the filtrate is reclaimed and returned to the blood. This selective transepithelial process ensures that essential nutrients, ions, and water are reabsorbed, while waste products are excreted.
Definition: Tubular reabsorption refers to the movement of substances from the filtrate in the renal tubules back into the blood of the peritubular capillaries.
Key Features: Almost all organic nutrients are reabsorbed; water and ion reabsorption are hormonally regulated and adjusted.
Routes: Substances can follow either the transcellular or paracellular route.
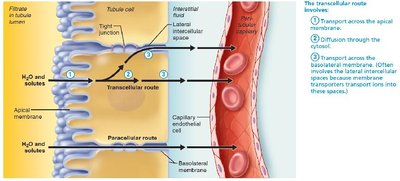
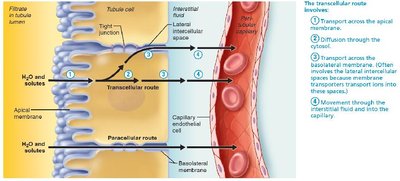
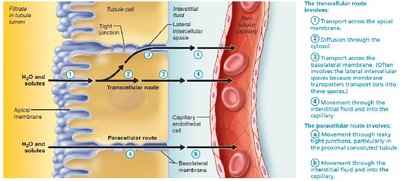
Transcellular and Paracellular Routes
Tubular reabsorption occurs via two main pathways:
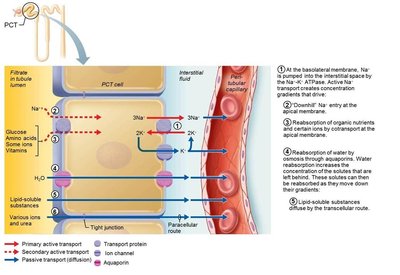
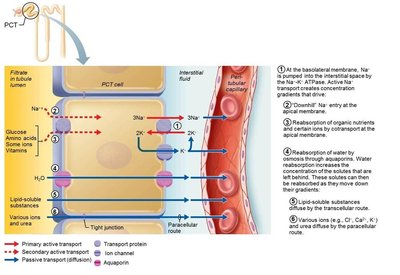
Transcellular Route: Solutes pass through the apical membrane, cytosol, and basolateral membrane of the tubule cell, then enter the blood through the endothelium of peritubular capillaries.
Paracellular Route: Solutes move between tubule cells, limited by tight junctions but leaky in the proximal nephron. Water, Ca2+, Mg2+, K+, and some Na+ in the PCT move via this route.
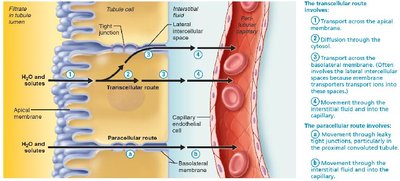
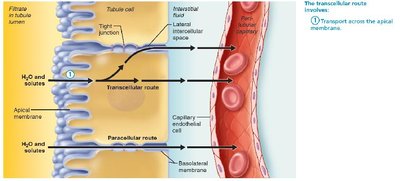
Stepwise Mechanism of Transcellular Route
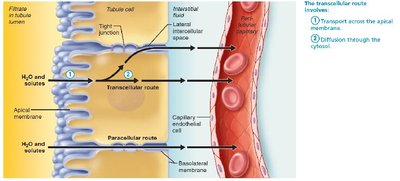
1. Transport across the apical membrane
2. Diffusion through the cytosol
3. Transport across the basolateral membrane
4. Movement through the interstitial fluid and into the capillary
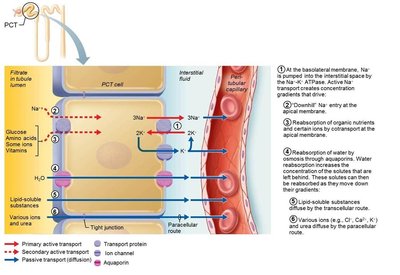
Tubular Reabsorption of Sodium
Sodium Transport Mechanisms
Sodium (Na+) is the most abundant cation in filtrate and its reabsorption is essential for the reabsorption of other substances.
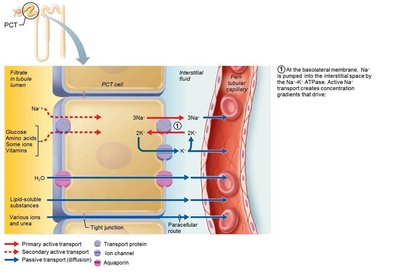
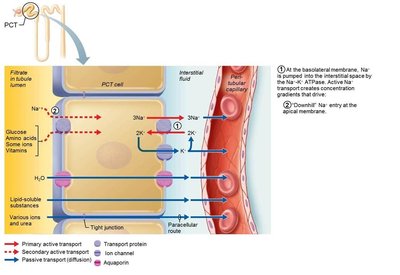
Basolateral Membrane: Na+ is transported via primary active transport using the Na+-K+ ATPase pump, which moves Na+ into the interstitial space.
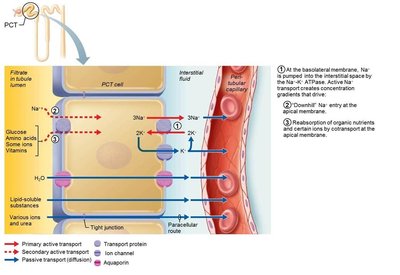
Apical Membrane: Na+ enters tubule cells via secondary active transport (cotransport) or facilitated diffusion through channels.
Electrochemical Gradient: Active pumping of Na+ at the basolateral membrane creates a strong gradient, facilitating Na+ diffusion into the cell.
Tubular Reabsorption of Nutrients, Water, and Ions
Mechanisms and Regulation
The reabsorption of nutrients, water, and ions is closely linked to Na+ transport and involves both active and passive mechanisms.
Secondary Active Transport: Organic nutrients (glucose, amino acids, some ions, vitamins) are cotransported with Na+.
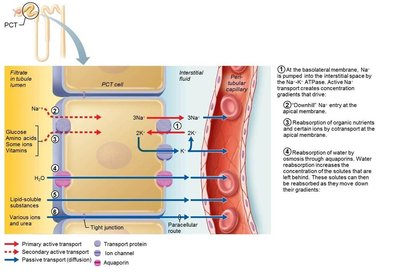
Passive Reabsorption of Water: Movement of Na+ and other solutes creates an osmotic gradient for water, which is reabsorbed by osmosis through aquaporins.
Obligatory Water Reabsorption: Aquaporins are always present in the PCT.
Facultative Water Reabsorption: Aquaporins are inserted in collecting ducts only if ADH is present.
Passive Reabsorption of Solutes: As water is reabsorbed, solute concentration increases, driving their entry into tubule cells and capillaries.
Transport Maximum (Tm)
Concept and Clinical Relevance
Transcellular transport systems are specific and limited, with a transport maximum (Tm) for each reabsorbed substance.
Definition: Tm reflects the number of carriers available in renal tubules.
Clinical Example: Hyperglycemia leads to high blood glucose levels that exceed Tm, causing glucose to spill into urine.
Reabsorptive Capabilities of Renal Tubules and Collecting Ducts
Segmental Functions
Different segments of the nephron have specialized reabsorptive capabilities.
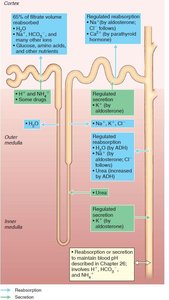
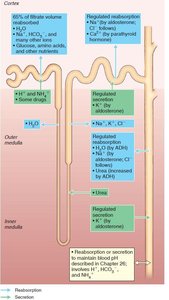
Proximal Convoluted Tubule (PCT): Site of most reabsorption; all nutrients, 65% of Na+ and water, many ions, almost all uric acid, and about half of urea are reabsorbed.
Nephron Loop: Descending limb allows water to leave, ascending limb allows solutes to leave.
Distal Convoluted Tubule (DCT) and Collecting Duct: Reabsorption is hormonally regulated (ADH, aldosterone, atrial natriuretic peptide, parathyroid hormone).
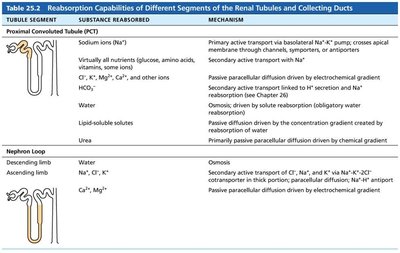
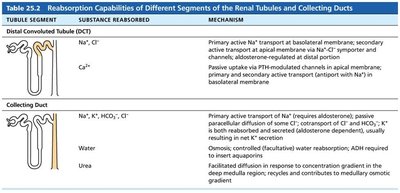
Tubule Segment | Substance Reabsorbed | Mechanism |
|---|---|---|
Proximal Convoluted Tubule (PCT) | Sodium ions, virtually all nutrients, water, lipid-soluble solutes, urea | Primary active transport, secondary active transport, osmosis, passive diffusion |
Nephron Loop | Descending limb: water; Ascending limb: Na+, Cl-, Ca2+ | Osmosis, secondary active transport, passive diffusion |
Distal Convoluted Tubule (DCT) | Na+, Cl-, Ca2+ | Primary and secondary active transport, passive uptake |
Collecting Duct | Na+, K+, HCO3-, Cl-, water, urea | Primary active transport, passive diffusion, osmosis, facilitated diffusion |
Tubular Secretion
Mechanism and Importance
Tubular secretion is the process of moving substances from the blood into the filtrate, primarily in the PCT.
Definition: Tubular secretion is reabsorption in reverse, moving selected substances from peritubular capillaries through tubule cells into the filtrate.
Substances Secreted: K+, H+, NH4+, creatinine, organic acids and bases, and substances synthesized in tubule cells (e.g., HCO3-).
Functions: Disposes of bound substances, eliminates undesirable substances, rids body of excess K+, and controls blood pH.
Regulation of Urine Concentration and Volume
Osmolality and Countercurrent Mechanisms
The kidneys regulate urine concentration and volume to maintain body fluid osmotic concentration at around 300 mOsm.
Osmolality: Number of solute particles in 1 kg of H2O; body fluids are measured in milliosmols (mOsm).
Countercurrent Mechanism: Fluid flows in opposite directions in adjacent segments of the nephron loop, creating and maintaining a medullary osmotic gradient.
Types: Countercurrent multiplier (nephron loop) and countercurrent exchanger (vasa recta).

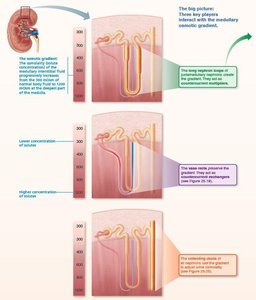
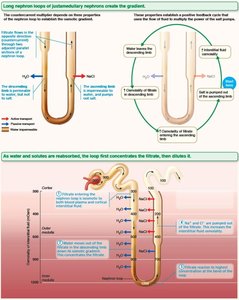
Countercurrent Multiplier
Ascending Limb: Impermeable to water, selectively permeable to solutes; Na+ and Cl- are actively reabsorbed.
Descending Limb: Freely permeable to water, impermeable to solutes; water leaves filtrate, increasing osmolality.
Mechanism: The more NaCl the ascending limb transports, the more water diffuses out of the descending limb, multiplying the gradient along the loop.
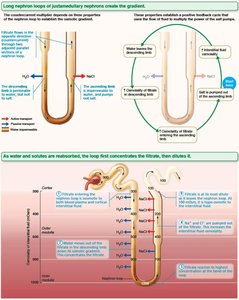
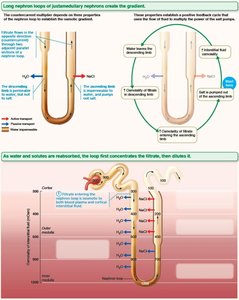
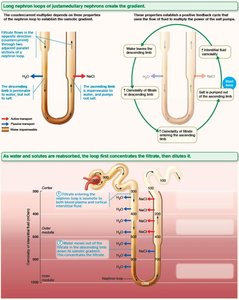
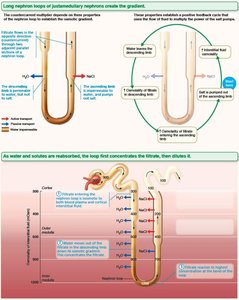
Countercurrent Exchanger
Vasa Recta: Highly permeable to water and solutes; blood flow is countercurrent, allowing exchange without disrupting the gradient.
Preservation: Prevents rapid removal of salt and removes reabsorbed water, maintaining the medullary gradient.
Formation of Dilute or Concentrated Urine
Mechanisms and Clinical Relevance
The established medullary osmotic gradient allows the kidney to produce urine of varying concentration, depending on hydration status and hormone levels.
Overhydration: Produces large volume of dilute urine; ADH decreases, urine ~100 mOsm.
Dehydration: Produces small volume of concentrated urine; maximal ADH released, urine ~1200 mOsm.
Urea Recycling and Medullary Osmotic Gradient
Role of Urea
Urea contributes to the medullary gradient by recycling between the nephron loop and collecting duct, increasing osmolality in the medulla.
Urea enters filtrate in the ascending thin limb by facilitated diffusion.
Water reabsorption in the collecting duct leaves urea behind, which then diffuses into the medulla.
Clinical Evaluation of Kidney Function
Urinalysis and Renal Clearance
Urinalysis: Examines urine for signs of disease or illegal substances.
Renal Clearance: Volume of plasma kidneys can clear of a substance per unit time; used to determine GFR and detect renal disease.
Formula: Where: C = renal clearance rate (ml/min) U = concentration of substance in urine (mg/ml) V = flow rate of urine formation (ml/min) P = concentration of substance in plasma (mg/ml)
Urine Composition and Characteristics
Chemical and Physical Properties
Chemical Composition: 95% water, 5% solutes (urea, uric acid, creatinine, ions).
Physical Characteristics: Color (clear to deep yellow), odor (aromatic, ammonia upon standing), pH (slightly acidic, ~6), specific gravity (1.001–1.035).
Transport, Storage, and Elimination of Urine
Ureters, Bladder, and Urethra
Ureters: Convey urine from kidneys to bladder; three layers (mucosa, muscularis, adventitia).
Bladder: Muscular sac for temporary storage; layers include mucosa, detrusor muscle, and adventitia.
Urethra: Muscular tube draining bladder; internal and external sphincters control flow.
Micturition (Urination)
Control and Reflexes
Three events: contraction of detrusor (ANS), opening of internal sphincter (ANS), opening of external sphincter (somatic NS).
Reflexive urination in infants; voluntary control develops with nervous system maturation.
Developmental Aspects and Clinical Imbalances
Embryonic Development and Common Disorders
Three sets of embryonic kidneys: pronephros, mesonephros, metanephros (adult kidney).
Congenital abnormalities: horseshoe kidney, hypospadias, polycystic kidney disease.
Frequent micturition in infants, incontinence, and age-related changes in kidney function.
