 Back
BackType 1 Diabetes Mellitus: Pathophysiology, Clinical Manifestations, and Management
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Type 1 Diabetes Mellitus
Overview
Type 1 diabetes mellitus (T1DM) is a chronic autoimmune disorder characterized by the destruction of pancreatic beta cells, resulting in absolute insulin deficiency. This condition primarily affects children and young adults but can occur at any age. Effective management requires a comprehensive understanding of its pathophysiology, clinical manifestations, and therapeutic interventions.
Role of Pancreatic Hormones in Metabolism
Pancreatic Cell Types and Their Functions
Alpha Cells: Produce glucagon, which stimulates gluconeogenesis (synthesis of glucose from non-carbohydrate sources), glycogenolysis (breakdown of glycogen to glucose), and lipolysis (breakdown of lipids to fatty acids).
Beta Cells: Produce insulin, which facilitates glucose uptake into cells, inhibits excessive glycogen breakdown, and regulates blood glucose levels.
Delta Cells: Produce somatostatin, which inhibits the secretion of both insulin and glucagon and slows gastric motility.
Etiology, Risk Factors, and Prevention
Etiology
Autoimmune destruction of pancreatic beta cells
Genetic predisposition (HLA genes)
Environmental triggers (e.g., viral infections)
Risk Factors
Family history of type 1 diabetes
Presence of other autoimmune diseases
Geographic and ethnic variations
Prevention
No known preventive measures for type 1 diabetes due to its autoimmune nature
Pathophysiology of Type 1 Diabetes Mellitus
In T1DM, the immune system targets and destroys insulin-producing beta cells in the pancreas. This leads to an absolute deficiency of insulin, resulting in hyperglycemia and impaired metabolism of carbohydrates, proteins, and fats.
Clinical Manifestations
Polyuria (frequent urination)
Polydipsia (excessive thirst)
Polyphagia (increased hunger)
Weight loss
Fatigue
Blurred vision
Acute Complications
Diabetic Ketoacidosis (DKA)
Life-threatening complication due to insulin deficiency
Characterized by hyperglycemia, ketosis, metabolic acidosis, and dehydration
Symptoms: Nausea, vomiting, abdominal pain, rapid breathing, fruity breath odor
Hypoglycemia
Low blood glucose, often due to excess insulin or missed meals
Symptoms: Shakiness, sweating, confusion, irritability, loss of consciousness
Dawn Phenomenon
Early morning rise in blood glucose due to hormonal changes
Somogyi Phenomenon
Rebound hyperglycemia following nocturnal hypoglycemia
Chronic Complications
Microvascular Complications
Retinopathy (eye damage)
Nephropathy (kidney damage)
Neuropathy (nerve damage)
Macrovascular Complications
Cardiovascular disease
Peripheral arterial disease
Stroke
Diagnostic Tests
Fasting Plasma Glucose (FPG): Measures blood glucose after fasting
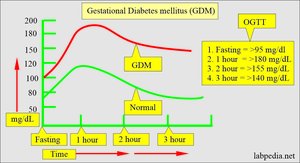
Oral Glucose Tolerance Test (OGTT): Assesses glucose handling after a glucose load
A1C: Reflects average blood glucose over 2-3 months
Lipid Profile: Evaluates cardiovascular risk
Creatinine, Albumin/Creatinine Ratio, GFR: Assess kidney function
Ketones: Detects diabetic ketoacidosis
Electrolytes: Monitors metabolic status
Monitoring Blood Glucose
Self-monitoring of blood glucose (SMBG) is essential for adjusting therapy and preventing complications.
Continuous glucose monitoring (CGM) systems provide real-time data.
Pharmacologic Therapy
Types of Insulin
Rapid-acting: Insulin aspart (Novolog), insulin lispro (Humalog)
Short-acting: Regular insulin
Intermediate-acting: NPH insulin
Long-acting: Insulin glargine (Lantus)

Type | Name | Onset (H) | Peak (H) | Duration (H) |
|---|---|---|---|---|
Rapid-acting | aspart (Novolog), lispro (Humalog) | 0.25 | 0.5-1.5 | 3-5 |
Short-acting | regular | 0.5-1 | 2-4 | 4-6 |
Intermediate-acting | NPH | 2 | 6-8 | 12-16 |
Long-acting | glargine (Lantus) | 2 | no peak | 24+ |


Nutrition Management
Balanced diet with controlled carbohydrate intake
Consistent meal timing to match insulin action
Monitoring of blood glucose response to foods
Sick Day Management
Monitor blood glucose every 3-4 hours
Continue long-acting or basal insulin
Monitor urine for ketones
Maintain hydration with fluids (water, tea, broth)
Consume carbohydrates to prevent hypoglycemia
Contact healthcare provider if vomiting, diarrhea, or fever persists for more than 6 hours or if blood glucose remains >240 mg/dL
Exercise
Consult healthcare provider before starting a new exercise program
Monitor blood glucose before, during, and after exercise
May require increased carbohydrate intake before activity
Maintain adequate fluid intake

Lifespan Considerations
Children and Adolescents
Growth and hormonal changes affect insulin needs
Education for self-management is crucial
Pregnant Women
Strict glycemic control to prevent complications for mother and fetus
Older Adults
Increased risk of hypoglycemia and comorbidities
Individualized treatment goals
Nursing Process in Type 1 Diabetes Care
Assessment
Comprehensive patient interview and physical assessment
Evaluation of self-care abilities and support systems
Diagnosis
Identify actual and potential health problems related to diabetes
Planning
Set individualized, measurable goals for glycemic control and complication prevention
Implementation
Administer medications, provide education, and coordinate care
Evaluation
Assess achievement of goals and modify care as needed
Sample NCLEX Questions
What is the priority nursing concern for a client with diabetes who walks barefoot after angioplasty?
Potential for infection from microtrauma while walking barefoot
What is the priority action for a diabetic client with a headache, moist hands, and missed breakfast?
Check the blood glucose level and be prepared to give 4 ounces of juice immediately.
Additional info: This guide integrates foundational pathophysiology, clinical features, and management strategies for type 1 diabetes mellitus, as well as relevant nursing considerations and sample exam questions for comprehensive review.
