 Back
BackUrinary System: Tubular Reabsorption and Secretion
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Urinary System: Tubular Reabsorption and Secretion
Overview of Nephron Function
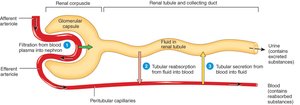
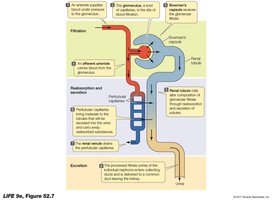
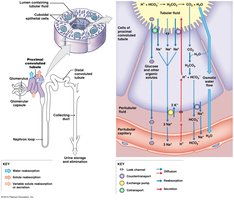
The nephron is the functional unit of the kidney, responsible for filtering blood and forming urine. The main processes include glomerular filtration, tubular reabsorption, and tubular secretion, which together regulate the volume and composition of body fluids.
Glomerular Filtration: Blood pressure forces water and solutes across the glomerular capillaries into the nephron, forming filtrate.
Tubular Reabsorption: Useful substances are reclaimed from the filtrate and returned to the blood.
Tubular Secretion: Additional wastes and excess ions are secreted from the blood into the tubular fluid for excretion.
Glomerular Filtration
Filtration occurs in the renal corpuscle, where plasma is filtered from the glomerulus into the capsular space. This process is non-selective and driven by hydrostatic pressure.
Filtrate: Contains water, ions, glucose, amino acids, and small molecules, but excludes large proteins and blood cells.
Filtration Rate: The glomerular filtration rate (GFR) is the volume of filtrate formed per minute by both kidneys, typically about 125 mL/min in adults.
Tubular Reabsorption
General Principles
Tubular reabsorption is the process by which the nephron removes water and solutes from the tubular fluid and returns them to the blood. This is essential for conserving nutrients and maintaining fluid and electrolyte balance.
Sites: Most reabsorption occurs in the proximal convoluted tubule (PCT), with fine-tuning in the nephron loop, distal convoluted tubule (DCT), and collecting duct.
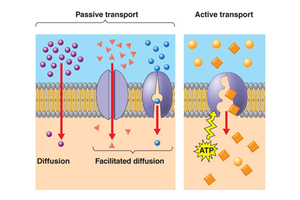
Mechanisms: Includes active transport, facilitated diffusion, osmosis, and pinocytosis for small proteins.
Volume: About 99% of the filtrate is reabsorbed; only 1% becomes urine.

Mechanisms of Transport
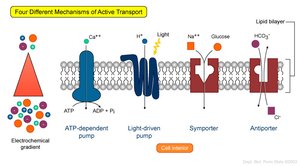
Carrier-mediated transport is crucial for reabsorption and secretion. It includes several types:
Facilitated Diffusion: Movement of substances down their concentration gradient via carrier proteins.
Active Transport: Movement against a gradient using ATP.
Cotransport (Symport): Two substances move in the same direction across the membrane.
Countertransport (Antiport): Two substances move in opposite directions.
Carrier-Mediated Transport Characteristics
Specificity: Each carrier protein transports specific substances.
Unidirectionality: Most carriers move substances in one direction only.
Distribution: Carrier proteins are unevenly distributed along the nephron.
Saturation: There is a maximum rate of transport (Tm), beyond which carriers are saturated and excess solute appears in urine.
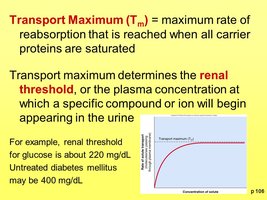
Transport Maximum and Renal Threshold
The transport maximum (Tm) is the maximum rate at which a substance can be reabsorbed. When plasma concentration exceeds the renal threshold, the substance appears in urine.
Example: Glucose has a renal threshold of about 220 mg/dL. Above this, glucose appears in urine (glucosuria).

Reabsorption in the Proximal Convoluted Tubule (PCT)
The PCT is responsible for the majority of solute and water reabsorption. Most processes involve sodium (Na+) transporters.
Reabsorbs over 99% of organic nutrients (glucose, amino acids), 80-90% of bicarbonate (HCO3-), 65% of water, Na+, and K+, 50% of Cl-, and variable amounts of Ca2+, Mg2+, and HPO42-.
Secretes H+ ions to help regulate blood pH.


Five Functions of the PCT
Reabsorption of organic nutrients
Active reabsorption of ions
Reabsorption of water
Passive reabsorption of ions
Secretion of H+ ions
Nephron Loop (Loop of Henle)
Descending and Ascending Limbs
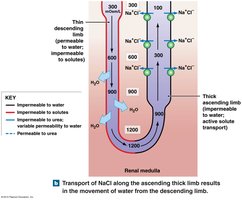
The nephron loop has distinct permeability characteristics that enable the concentration of urine through countercurrent multiplication.
Descending Limb: Permeable to water, impermeable to solutes. Water exits by osmosis.
Ascending Limb: Impermeable to water, actively transports Na+ and Cl- out of the tubule.

Countercurrent Multiplication
This process refers to the interaction between the descending and ascending limbs, which creates a concentration gradient in the medulla, allowing for efficient reabsorption of water and solutes.
Establishes a gradient for water reabsorption in the collecting duct, regulated by antidiuretic hormone (ADH).
Distal Convoluted Tubule (DCT) and Collecting Duct
Reabsorption and Secretion in the DCT
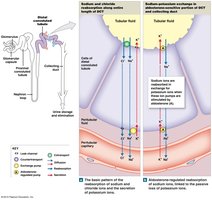
The DCT continues to reabsorb Na+ and Cl- via cotransporters and is a major site for hormonal regulation of ion balance.
Aldosterone: Increases Na+ reabsorption and K+ secretion.
Parathyroid Hormone (PTH): Stimulates Ca2+ reabsorption.
DCT is relatively impermeable to water unless ADH is present.
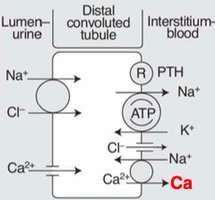
Secretion in the DCT
Secretes K+ and H+ ions, with rates depending on their concentrations in the peritubular fluid.
H+ secretion is coupled with Na+ reabsorption, helping to regulate blood pH.
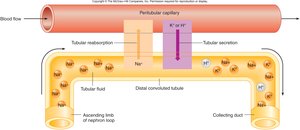
Collecting Duct: Final Adjustments
The collecting duct makes the final adjustments to urine composition, including reabsorption of water (regulated by ADH), sodium, bicarbonate, and urea, and secretion of H+ or HCO3- to control pH.
By the end of the DCT, 95% of solutes and water have been reabsorbed.
Intercalated cells in the collecting duct secrete H+ via proton pumps and reabsorb bicarbonate via Cl-/HCO3- exchangers.
Urine is buffered by phosphate and ammonia.


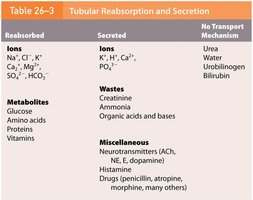
Summary Table: Tubular Reabsorption and Secretion
Reabsorbed | Secreted | No Transport Mechanism |
|---|---|---|
Ions: Na+, Cl-, K+, Ca2+, Mg2+, SO42-, HCO3- Metabolites: Glucose, amino acids, proteins, vitamins | Ions: K+, H+, Ca2+, PO43- Wastes: Creatinine, ammonia, organic acids and bases Miscellaneous: Neurotransmitters, histamine, drugs | Urea, water, urobilinogen, bilirubin |
Summary of Water Reabsorption
PCT: 65%
Nephron loop: 15%
DCT: 10-15%
Collecting duct: 5-10%
