 Back
BackUrinary System: Tubular Reabsorption, Secretion, and Regulation of Urine Concentration
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Urinary System: Tubular Reabsorption, Secretion, and Regulation
Overview of the Urinary System
The urinary system is essential for filtering blood, removing waste, and maintaining fluid, electrolyte, and acid-base balance. The nephron is the functional unit of the kidney, responsible for filtration, reabsorption, and secretion.

Tubular Reabsorption
Tubular reabsorption is the process by which the nephron removes water and solutes from the tubular fluid and returns them to the blood. This process is highly selective and critical for conserving essential substances.
Selective Process: Almost all organic nutrients are reabsorbed; water and ion reabsorption are hormonally regulated and adjusted.
Active and Passive Reabsorption: Includes both energy-requiring (active) and energy-independent (passive) mechanisms.

Reabsorption of Sodium (Na+)
Primary Active Transport: Sodium is the most abundant cation in filtrate. Na+ is transported across the tubule cell membrane via the Na+-K+ ATPase pump, which moves Na+ into the interstitial space, from where it is swept into peritubular capillaries.
Secondary Active Transport: The electrochemical gradient created by Na+ movement provides the energy for the co-transport of other solutes, such as glucose, amino acids, and some ions and vitamins.

Reabsorption of Water
Osmotic Gradient: Movement of Na+ and other solutes creates an osmotic gradient for water, which is reabsorbed by osmosis through aquaporins (water channels).
Obligatory Water Reabsorption: Aquaporins are always present in the proximal convoluted tubule (PCT).
Facultative Water Reabsorption: Aquaporins are inserted in the collecting ducts only if antidiuretic hormone (ADH) is present.

Passive Reabsorption of Solutes
As water is reabsorbed, the concentration of solutes in the filtrate increases, creating gradients for passive reabsorption of fat-soluble substances, some ions, and urea.
Transport Maximum (Tm)
Each reabsorbed substance has a transport maximum, which is the maximum rate at which it can be reabsorbed. When carriers are saturated, excess solute is excreted in urine (e.g., glucose in diabetes).

Reabsorption in Different Nephron Segments
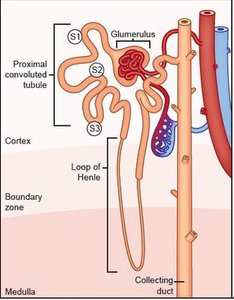
Proximal Convoluted Tubule (PCT): Site of most reabsorption (all nutrients, 65% of Na+ and water, many ions, almost all uric acid, about half of urea).
Nephron Loop (Loop of Henle): Descending limb is permeable to water but not solutes; ascending limb is impermeable to water but allows solute reabsorption (thin segment passive to Na+, thick segment actively transports Na+).
Distal Convoluted Tubule (DCT) and Collecting Duct: Reabsorption is hormonally regulated (ADH increases water reabsorption, aldosterone increases Na+ reabsorption, atrial natriuretic peptide decreases Na+ reabsorption, parathyroid hormone increases Ca2+ reabsorption).
Tubular Secretion
Tubular secretion is the process of moving substances from the blood into the filtrate. It is essentially reabsorption in reverse and occurs mainly in the PCT.
Substances Secreted: K+, H+, NH4+, creatinine, organic acids and bases, and substances synthesized in tubule cells (e.g., HCO3–).
Functions: Disposing of substances bound to plasma proteins (e.g., drugs), eliminating undesirable substances (e.g., urea, uric acid), ridding the body of excess K+ (aldosterone effect), and controlling blood pH by altering H+ or HCO3– in urine.
Regulation of Urine Concentration and Volume
The kidneys maintain body fluid osmotic concentration at around 300 mOsm by adjusting urine concentration and volume using countercurrent mechanisms.
Osmolality: Number of solute particles in 1 kg of H2O.
Countercurrent Mechanism: Fluid flows in opposite directions in two adjacent segments of the same tube with a hairpin turn, allowing efficient exchange and gradient formation.
Countercurrent Multiplier: Interaction of filtrate flow in ascending/descending limbs of nephron loops (juxtamedullary nephrons) creates the medullary osmotic gradient.
Countercurrent Exchanger: Blood flow in ascending/descending limbs of vasa recta preserves the gradient.
Formation of Dilute or Concentrated Urine
Overhydration: Produces large volume of dilute urine; ADH production decreases, urine osmolality ~100 mOsm.
Dehydration: Produces small volume of concentrated urine; maximal ADH is released, urine osmolality ~1200 mOsm.
Urea Recycling
Urea helps form the medullary gradient by cycling between the collecting duct and the nephron loop, contributing to high osmolality in the medulla.
Diuretics
Definition: Chemicals that enhance urinary output.
Types: ADH inhibitors (e.g., alcohol), Na+ reabsorption inhibitors (e.g., caffeine, some drugs), loop diuretics (inhibit medullary gradient formation), and osmotic diuretics (substances not reabsorbed, e.g., glucose in diabetes).
Renal Failure
Definition: GFR < 15 ml/min, leading to uremia (ionic and hormonal imbalances, metabolic abnormalities, toxic molecule accumulation).
Symptoms: Fatigue, anorexia, nausea, mental changes, cramps.
Treatment: Hemodialysis or transplant.
Composition and Characteristics of Urine
Chemical Composition: 95% water, 5% solutes (urea, uric acid, creatinine, Na+, K+, PO43–, SO42–, Ca2+, Mg2+, HCO3–).
Abnormal Constituents: Blood proteins, WBCs, bile pigments may indicate disease.
Physical Characteristics: Clear, pale to deep yellow (urochrome pigment), slightly aromatic, pH ~6 (range 4.5–8.0), specific gravity 1.001–1.035.
Transport, Storage, and Elimination of Urine
Ureters: Slender tubes conveying urine from kidneys to bladder; prevent backflow by closing as bladder pressure increases.
Renal Calculi (Kidney Stones): Crystallized calcium, magnesium, or uric acid salts; may block ureter, causing pain and pressure. Treatment includes shock waves, surgery, hydration, and pain management.
Urinary Bladder: Muscular sac for temporary urine storage; can hold ~500 ml, up to twice as much if necessary.
Urethra: Muscular tube draining the bladder.
Micturition (Urination)
Involves contraction of bladder muscle (ANS), opening of internal urethral sphincter (ANS), and opening of external urethral sphincter (somatic nervous system).
Age-Related Changes
Kidneys shrink, nephrons decrease in size and number, tubule cells become less efficient.
By age 80, GFR is half that of a young adult; nocturia and incontinence are common due to bladder shrinkage and loss of tone.
Table: Reabsorption Capabilities of Renal Tubule Segments
Segment | Substances Reabsorbed | Regulation |
|---|---|---|
Proximal Convoluted Tubule (PCT) | All nutrients, 65% Na+ and water, many ions, almost all uric acid, ~50% urea | Obligatory |
Nephron Loop (Descending Limb) | Water | Obligatory |
Nephron Loop (Ascending Limb) | Na+, Cl–, K+ | Obligatory |
Distal Convoluted Tubule (DCT) & Collecting Duct | Water, Na+, Cl–, Ca2+, urea | Hormonally regulated (ADH, aldosterone, PTH, ANP) |
Additional info: This summary integrates textbook-level explanations and organizes the nephron's processes for exam preparation. Only images directly illustrating nephron structure, reabsorption, and regulatory mechanisms are included for clarity.
