 Back
BackPhospholipids, Glycosphingolipids, and Cholesterol: Structure, Function, and Clinical Relevance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Phospholipids, Glycosphingolipids, and Cholesterol
Overview
This section explores the structure, synthesis, and physiological roles of major membrane lipids—phospholipids, glycosphingolipids, and cholesterol. These molecules are essential for membrane structure, cellular signaling, and serve as precursors for important biomolecules. Their clinical significance is highlighted in disorders such as respiratory distress syndrome and lipid storage diseases.
Phospholipids
Structure and Types
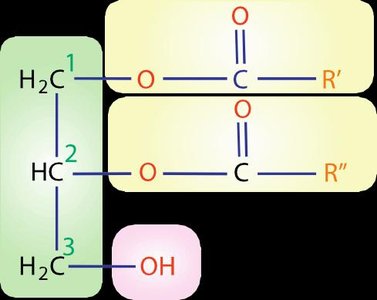
Phospholipids are amphipathic molecules, meaning they contain both hydrophilic (water-loving) and hydrophobic (water-fearing) regions. They are major constituents of biological membranes and play key roles in membrane structure and function.
Glycerolipids: Built on a glycerol backbone. Major types include:
Phosphatidylcholine (Lecithin): Glycerol + phosphate + choline
Phosphatidylethanolamine (Cephalin): Glycerol + phosphate + ethanolamine
Phosphatidylserine: Glycerol + phosphate + serine
Phosphatidylinositol: Glycerol + phosphate + inositol
Phosphatidylglycerol: Glycerol + phosphate + glycerol
Cardiolipin: Diphosphatidylglycerol, unique to the inner mitochondrial membrane and antigenic
Sphingolipids: Contain a sphingosine backbone. The main type in humans is sphingomyelin (ceramide + phosphorylcholine), a key component of myelin sheaths in nerve fibers.
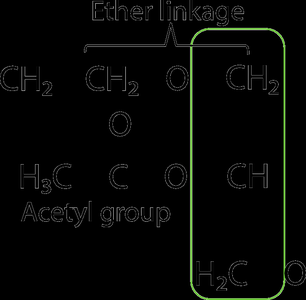
Platelet-Activating Factor (PAF)
PAF is an ether phospholipid with potent biological activity, involved in inflammation and platelet aggregation.
Glycosphingolipids
Structure and Function
Glycosphingolipids are sphingolipids with attached carbohydrate groups. They are important for cell recognition, signal transduction, and membrane stability. Storage disorders can result from defects in their breakdown, leading to diseases such as Tay-Sachs and Gaucher disease.
Phospholipids and Glycosphingolipids in Clinical Medicine
Pulmonary Surfactant and Respiratory Distress Syndrome (RDS)
Pulmonary surfactant is a complex of lipids (90%) and proteins (5-10%) synthesized in alveolar type II cells. It reduces alveolar surface tension, preventing lung collapse during exhalation. The main lipid component is lecithin (phosphatidylcholine), with phosphatidylglycerol (PG), phosphatidylinositol (PI), phosphatidylethanolamine (PE), phosphatidylserine (PS), and cholesterol also present.
Immature surfactant: High in PI, PE, PS; low PG/PI ratio indicates lung immaturity.
RDS: Common in premature infants due to insufficient surfactant; leads to high neonatal mortality and morbidity.
ARDS: Acute respiratory distress syndrome in adults, often due to sepsis or trauma, involves surfactant dysfunction and is treated with surfactant and antiproteinases.
Biochemical Determinants of Fetal Lung Maturity
Lecithin/Sphingomyelin (L/S) Ratio: Used to assess fetal lung maturity in amniotic fluid. A ratio >2 indicates maturity; <1.5 suggests high risk of RDS.
Lamellar Body Count: >30,000-50,000/μL and optical density (OD) >0.15 indicate maturity.
Antioxidant Enzyme System: Includes superoxide dismutase, glutathione peroxidase, catalase, and other antioxidants (vitamin E, β-carotene, glutathione, cysteine). Premature infants are susceptible to deficiencies in both surfactant and antioxidant defenses.
Cholesterol
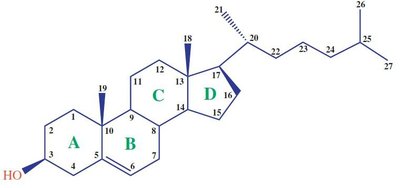
Structure and Function
Cholesterol is a sterol of animal origin, essential for membrane fluidity and precursor for bile acids, steroid hormones, and vitamin D. It exists in free and esterified forms and is transported in plasma via lipoproteins.
Synthesized by most tissues, especially liver, intestine, adrenal cortex, and reproductive tissues.
All carbon atoms are derived from acetate; NADPH provides reducing equivalents.
Cholesterol Synthesis and Regulation
Cholesterol synthesis is tightly regulated at multiple levels, including feedback inhibition and hormonal control. The rate-limiting step is catalyzed by HMG-CoA reductase.
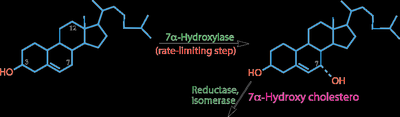
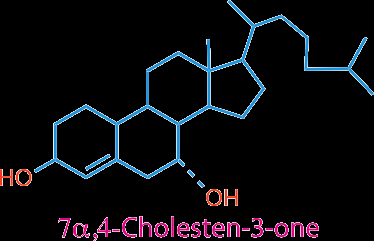
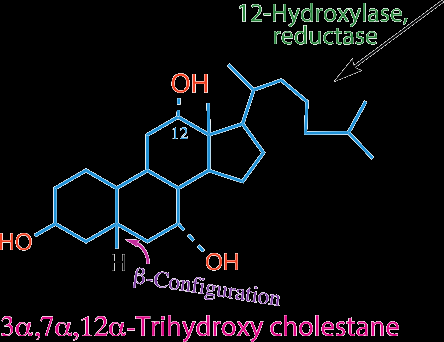
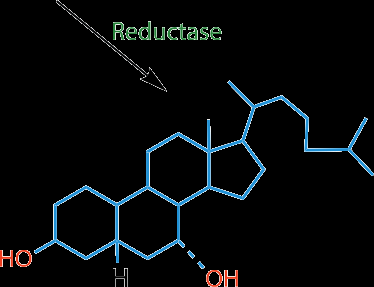
Bile Acids
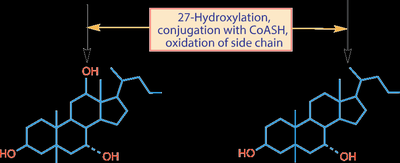
Formation and Types
Bile acids are synthesized from cholesterol in the liver and are critical for fat digestion and absorption. The main bile acids in humans are chenodeoxycholic acid (CDCA), cholic acid (CA), and deoxycholic acid (DCA, a secondary bile acid formed in the intestine).
About 2/3 of bile acids are derived from HDL cholesterol delivered to the liver.
Bile acids are conjugated with glycine or taurine to increase solubility.
Enterohepatic Circulation
Bile acids are secreted into the intestine, reabsorbed in the ileum, and returned to the liver via the portal circulation. This recycling is known as enterohepatic circulation.


Clinical Relevance of Bile Acid Metabolism
Serum bile acids: Sensitive indicator of liver disease; increased in hepatocellular disease and obstructive jaundice.
Lithocholic acid: Toxic, can cause hemolysis and fever.
Hyperbileacidemia: Causes pruritus, steatorrhea, hemolytic anemia, and further liver injury.
Cholelithiasis: Gallstone formation due to cholesterol precipitation in bile. A bile salt and phospholipid to cholesterol ratio <10:1 is lithogenic (stone-forming).
Pigment stones: Formed by elevated biliary pigments (bilirubin glucuronides).
Membrane Lipid Asymmetry
Maintenance of Asymmetry
Phospholipid asymmetry in membranes is maintained by specific enzymes:
Flippases: Move phospholipids from the outer to the inner leaflet.
Floppases: Move phospholipids from the inner to the outer leaflet.
Scramblases: Facilitate bidirectional movement, disrupting asymmetry during apoptosis or cell activation.
