 Back
BackComprehensive Study Notes on Reproductive and Maternal Health
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Reproductive Health and Maternal Well-being
Introduction to Reproductive Health
Reproductive health is a state of complete physical, mental, and social well-being in all matters relating to the reproductive system. It encompasses the ability to have a satisfying and safe sex life, the capability to reproduce, and the freedom to decide if, when, and how often to do so. Access to accurate information, safe and effective contraception, and skilled healthcare are essential for maintaining reproductive health.
Sexual and reproductive rights: Every individual has the right to make their own choices about their sexual and reproductive health.
Prevention: Includes contraception, prevention of sexually transmitted infections (STIs), and access to safe abortion care.
Empowerment: Informed individuals can protect themselves and make decisions about family planning and pregnancy.

Pregnancy: Phases, Changes, and Care
Physical and Psychological Changes During Pregnancy
Pregnancy is a period of significant physiological and psychological changes. These changes support fetal development and prepare the mother for childbirth and parenting.
Physical changes: Increased blood volume (up to 40%), heart rate, and cardiac output; physiological anemia; insulin resistance; increased glomerular filtration rate.
Psychological changes: Emotional fluctuations, anxiety, and decision-making challenges regarding birth and parenting.
Financial and social considerations: Planning for work, childcare, and family support.
Maternal Mortality and Its Causes
Maternal mortality refers to the death of a woman during pregnancy or within 42 days of termination, from causes related to or aggravated by pregnancy or its management. Deaths are classified as direct (resulting from obstetric complications) or indirect (due to pre-existing conditions exacerbated by pregnancy).
Direct causes: Hemorrhage, pre-eclampsia, thromboembolism, infection, obstructed labor, ectopic pregnancy, unsafe abortion, surgical and anesthetic complications.
Indirect causes: Pre-existing medical conditions (e.g., epilepsy, cardiac disease, diabetes), mental health issues, domestic violence, trauma.
Prevention: Most maternal deaths are preventable with skilled care during pregnancy, labor, and postpartum.

Barriers to Maternal Care
Barriers to accessing quality maternal care include poverty, distance, lack of information, inadequate services, and cultural practices. The "three delays" model identifies delays in seeking, reaching, and receiving care as critical contributors to maternal mortality.
Pregnancy Trimesters and Key Events
Pregnancy is divided into three trimesters, each with distinct physiological changes and potential complications.
First trimester (0-13 weeks): Early screening for fetal abnormalities, maternal infections, and rhesus status; common complications include miscarriage and ectopic pregnancy.
Second trimester (14-26 weeks): Nausea resolves, blood pressure falls, screening for gestational diabetes and anemia; complications include bleeding and infection.
Third trimester (27-40 weeks): Fetal growth, lung maturation, common symptoms include constipation and back pain; complications include infection, bleeding, and preeclampsia.

Prenatal and Antenatal Care
Prenatal care aims to ensure the health of both mother and baby through regular check-ups, screening, and education. WHO recommends at least 8 prenatal visits during pregnancy.
Screening: For pregnancy complications, anemia, infections, and fetal abnormalities.
Education: On healthy eating, exercise, and preparation for childbirth and parenthood.
Support: Emotional and psychological support for expectant mothers.

Family Planning and Preconception Care
Contraception and Birth Spacing
Family planning involves the use of contraception to prevent unwanted pregnancies and to space births for optimal maternal and child health. Access to safe abortion and post-abortion care is also essential.
Contraceptive methods: Include hormonal pills, intrauterine devices (IUDs), condoms, and injectables.
Preconception care: Management of pre-existing conditions, safe medication use, lifestyle changes, and vaccination.
Folic Acid and Neural Tube Defect Prevention
Folic acid supplementation before and during early pregnancy significantly reduces the risk of neural tube defects (NTDs) such as spina bifida and anencephaly.
Recommended dose: 400 μg daily for most women, 5 mg daily for high-risk groups (history of NTD, BMI >35, diabetes, epilepsy).
Timing: Begin supplementation 1-3 months prior to conception and continue through the first 12 weeks of pregnancy.

Gametogenesis: Spermatogenesis and Oogenesis
Spermatogenesis
Spermatogenesis is the process by which sperm are produced in the seminiferous tubules of the testes. It begins at puberty and continues throughout life.
Stages: Spermatogonia (stem cells) undergo mitosis, then meiosis to produce haploid spermatozoa.
Duration: Approximately 120 days for full maturation.
Normal sperm count: 15 million per mL; only a fraction are viable.

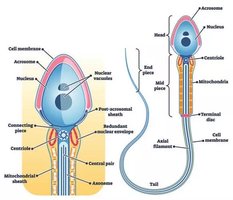
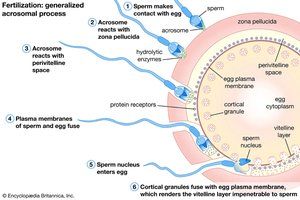
Sperm Structure and Function
The mature sperm consists of a head (containing DNA and acrosome), neck, and flagellum. The acrosome contains enzymes necessary for penetrating the oocyte's zona pellucida.
Capacitation: Occurs in the female reproductive tract, enabling the sperm to fertilize the oocyte.
Acrosome reaction: Releases enzymes to facilitate penetration of the oocyte.

Meiosis
Meiosis is a specialized cell division that reduces chromosome number by half, producing haploid gametes (sperm and eggs). In humans, somatic cells are diploid (2n), while gametes are haploid (n).
Process: Two rounds of division (meiosis I and II) yield four haploid cells from one diploid cell.
Importance: Maintains chromosome number across generations and introduces genetic diversity.
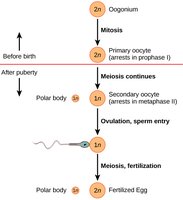
Oogenesis
Oogenesis is the process of egg (ovum) formation in females. It begins before birth, with primary oocytes arrested in prophase I until puberty. Each menstrual cycle, a few oocytes resume meiosis, but only one typically completes ovulation.
At birth: 1-2 million primary oocytes; by puberty, about 40,000 remain.
Hormonal regulation: FSH and LH from the anterior pituitary stimulate follicle development and ovulation.
Menstrual Cycle and Ovulation
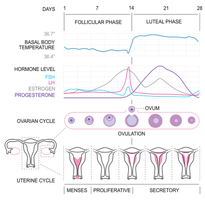
Phases of the Menstrual Cycle
The menstrual cycle averages 28 days and is divided into the follicular phase, ovulation, and luteal phase. Hormonal changes regulate the development and release of the egg and preparation of the endometrium for implantation.
Follicular phase (days 1-14): FSH stimulates follicle growth; estrogen thickens the endometrium.
Ovulation (day 14): LH surge triggers release of the oocyte.
Luteal phase (days 14-28): Corpus luteum secretes progesterone to maintain the endometrium.
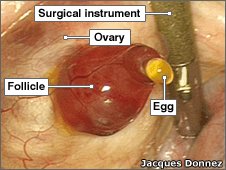
Ovulation and Fertilization
Ovulation is the release of a mature oocyte from the ovary, typically around day 14 of the cycle. Fertilization occurs in the fallopian tube when a sperm fuses with the oocyte, forming a zygote.
Key events: Estrogen peak, LH/FSH surge, follicle rupture, oocyte release, fimbriae guide egg into tube.
Fertilization steps: Sperm migration, zona pellucida penetration, membrane fusion, zygote formation.
Early Pregnancy and Placental Development
Implantation and Early Placenta
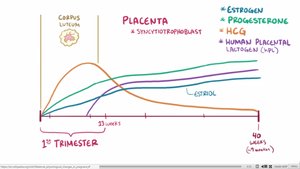
After fertilization, the zygote travels to the uterus and implants in the endometrium around day 8-9. The syncytiotrophoblast secretes human chorionic gonadotropin (hCG), which maintains the corpus luteum and supports early pregnancy.
Placenta: Fully developed by 13 weeks; functions in hormone production, nutrition, excretion, and immune protection.
Blood flow: At term, 600-700 mL/min flows through the placenta.
Hormonal Regulation in Pregnancy
Pregnancy-specific hormones maintain the uterine environment and support fetal development.
hCG: Maintains corpus luteum, supports progesterone production, and prevents menstruation.
Estrogen: Promotes uterine and breast growth, increases water retention, and prepares for labor.
Progesterone: Relaxes smooth muscle, prevents uterine contractions, and supports endometrial development.
Screening and Prevention in Pregnancy
Screening for Maternal and Fetal Health
Screening tests during pregnancy assess the risk of fetal abnormalities, maternal anemia, infections, and blood group incompatibilities. Early detection allows for timely interventions and informed decision-making.
Common screenings: Ultrasound (12-20 weeks), blood tests for anemia and infections, blood group and rhesus status.
Neural tube defects: Prevented by folic acid supplementation; screening identifies at-risk pregnancies.
Blood Groups and Rhesus Disease
Blood group and rhesus factor testing are essential in pregnancy to prevent hemolytic disease of the newborn. Rhesus-negative mothers carrying rhesus-positive babies may develop antibodies that attack fetal red blood cells in subsequent pregnancies.
Prevention: Anti-D immunoglobulin is given after sensitizing events to prevent antibody formation.

Summary Table: Key Maternal and Fetal Health Screenings
Screening/Test | Purpose | Timing |
|---|---|---|
Ultrasound | Fetal abnormalities, dating pregnancy | 12-20 weeks |
Blood group & Rhesus status | Prevent hemolytic disease | First prenatal visit |
Anemia screening | Detect maternal anemia | First visit, 28 weeks |
Infection screening | Rubella, Hepatitis B, HIV, Syphilis, Group B strep | First visit |
Gestational diabetes | Detect glucose intolerance | 24-28 weeks |
Conclusion
Understanding reproductive health, pregnancy physiology, and the importance of prenatal care is essential for personal and public health. Early screening, prevention, and education can significantly improve outcomes for mothers and babies.
