 Back
BackReproductive Health & Sexuality - Class 16
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Reproductive Health & Sexuality
Sexuality-Reproductive Pattern
The sexuality-reproductive pattern encompasses an individual's sexual self-concept, sexual functioning, methods of intimacy, and reproductive capacity. It is closely related to self-perception and relationship patterns, with body image, self-concept, role, and gender identity all contributing to sexual identity. Individual development and overall health influence reproductive capacity and sexual expression.
Sexual Self-Concept: How individuals perceive themselves as sexual beings, including their confidence and comfort with their sexuality.
Sexual Functioning: Refers to the physical, emotional, and psychological aspects of sexual activity and satisfaction.
Reproductive Patterns: Includes fertility, contraception, and pregnancy-related behaviors.
Assessment Objectives: Consider the continuum of sexual-identity expression and assess knowledge of sexual functioning and health practices (e.g., Pap smear, testicular self-examinations).
Adolescent Sexuality & Gender Identity
Adolescence is marked by the emergence of secondary sexual characteristics and sexual experimentation, which may involve heterosexual or same-sex activity. Anticipatory guidance is important for sexual decisions, contraception, and sexually transmitted blood-borne infection (STBBI) prevention. Adolescent pregnancy is associated with high risks for maternal and infant outcomes, as well as educational and economic effects. Support and services for pregnant adolescents are crucial for positive outcomes.
Gender Identity: Includes 2SLGBTQI+ individuals, with approximately 30% of Canadian youth identifying as such. These individuals experience higher rates of mood and anxiety disorders, poorer self-perceived health status, and higher risk of suicide.
Nurse’s Role: Creating a supportive, non-judgemental climate is essential for promoting health and well-being.
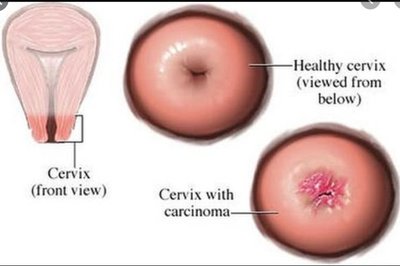
Cervical Cancer
Pathophysiology & Epidemiology
Cervical cancer develops at the squamocolumnar junction, where squamous epithelial cells (lining the outside of the cervix) meet columnar epithelial cells (lining the endocervix and uterus). Precursor lesions, such as high-grade cervical intraepithelial neoplasia (CIN), can progress to invasive cancer. In Canada, an estimated 1,650 women will be diagnosed with cervical cancer in 2025, with 430 deaths expected.
Precursor Lesions: High-grade CIN can progress to invasive cancer if not detected and treated.
Squamocolumnar Junction: The site where most cervical cancers originate.
Smoking & Cervical Cancer
Smoking doubles the risk of developing cervical cancer. Tobacco by-products are found in the cervical mucus of smokers, damaging or altering the DNA of healthy cervical cells and contributing to cancer development. Smoking also suppresses the immune system, making it harder for the body to clear infections and increasing the risk of recurrent low-grade lesions.
DNA Damage: Tobacco by-products directly damage cervical cells.
Immune Suppression: Reduced ability to clear HPV and other infections.
HPV: Human Papilloma Virus
HPV is a common group of viruses spread through skin-to-skin and sexual contact. Over 100 types exist, with 14 known to be oncogenic (cancer-causing). The immune system can clear most HPV strains, but aggressive strains are linked to genital warts and cancers such as throat, anal, and cervical cancer. Regular cervical screening detects changes caused by HPV, and vaccination is available to prevent infection.
Oncogenic HPV Strains: Types 16 and 18 are most aggressive and linked to cancer.
HPV Vaccination: Gardasil® and Gardasil-9 protect against multiple HPV strains.
Cervical Cancer: Risk & Preventative Factors
Risk factors for cervical cancer include lack of cervical screening, lack of follow-up care after abnormal screens, early age at first intercourse, multiple sexual partners, HPV infection, no HPV vaccination, history of genital warts, and smoking. Preventative factors include HPV vaccination, delaying intercourse, reducing the number of sexual partners, using barrier methods of contraception, and smoking cessation.
Primary Prevention: HPV vaccination via public health and school programs.
Secondary Prevention: Cervical screening for eligible females.
Tertiary Prevention: Timely treatment of positive screen test results.

HPV Vaccination in Newfoundland & Labrador (NL)
Gardasil® vaccination was initiated for girls in 2007, with a catch-up program for those born in 1994. In 2017, vaccination for boys began, but no catch-up was offered. Newcomers to NL born in 1994 or later are eligible for vaccination. NL has the highest vaccination rates in Canada.
Gardasil-9: Effective against 9 HPV strains (6, 11, 16, 18, 31, 33, 45, 52, 58).
Administration: Typically given in sixth grade, 2 doses over 6 months.
Cervical Cancer Screening
Screening Principles & Guidelines
Screening involves testing individuals of average risk with no symptoms to allow for early detection, treatment, and management of disease. Positive screening results lead to further testing and diagnosis. The goals of screening are to reduce disease-specific incidence and mortality, confirm the absence of disease, detect early disease, improve patient outcomes, and lower health care costs.
Routine Pap Testing: Recommended for women 21 years and older who are sexually active. Annual screening for three years; if all tests are negative, extend to every three years. Screening may cease at age 65 if there is a history of regular and negative Pap tests.
ASCUS-HPV Negative: Women 30 years and older with this result continue with routine screening.
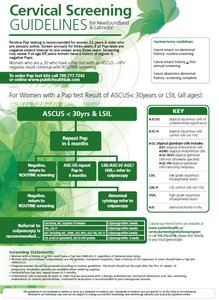
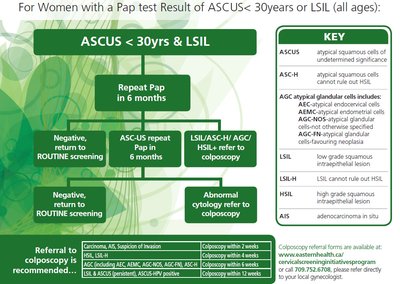
Cervical Screening: Abnormal Results
Abnormal Pap test results require follow-up, which may include repeat testing or referral to colposcopy. The guidelines provide a flowchart for managing ASCUS (atypical squamous cells of undetermined significance) and LSIL (low-grade squamous intraepithelial lesion) results.
Repeat Pap: If ASCUS or LSIL is detected, repeat Pap in 6 months.
Referral to Colposcopy: If abnormal cytology persists or higher-grade lesions are detected.
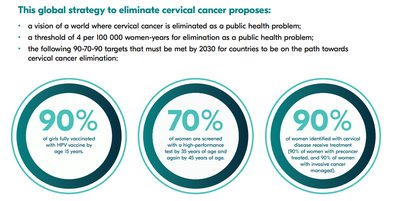
Global Strategies to End Cervical Cancer
WHO & CPAC Initiatives
The World Health Organization (WHO) and Canadian Partnership Against Cancer (CPAC) have launched global strategies to eliminate cervical cancer as a public health problem. The vision is to achieve a threshold of 4 per 100,000 women-years for elimination, with 90-70-90 targets to be met by 2030.
90%: Girls fully vaccinated with HPV vaccine by age 15.
70%: Women screened with a high-performance test by age 35 and again by age 45.
90%: Women identified with cervical disease receive treatment.

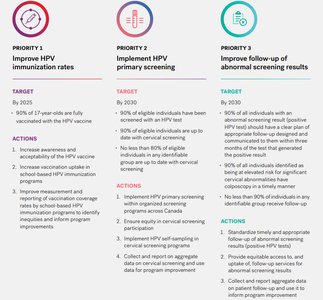
CPAC Priorities for Cervical Cancer Elimination
CPAC outlines three main priorities: improving HPV immunization rates, implementing HPV primary screening, and improving follow-up of abnormal screening results. Each priority has specific targets and actions to achieve by 2025 and 2030.
Priority 1: Increase HPV immunization rates among 17-year-olds.
Priority 2: Implement HPV primary screening for eligible individuals.
Priority 3: Improve follow-up of abnormal screening results to ensure timely and appropriate care.
Summary Table: Cervical Cancer Risk & Prevention
Risk Factors | Preventative Factors |
|---|---|
Lack of cervical screening | HPV vaccination (Gardasil®) |
Lack of follow-up care | Delay of intercourse |
Early age at first intercourse | Reduce number of sexual partners |
Multiple sexual partners | Barrier methods of contraception |
HPV infection | Smoking cessation |
No HPV vaccination | |
History of genital warts | |
Smoking |
Key Terms & Definitions
Cervical Intraepithelial Neoplasia (CIN): Pre-cancerous changes in the cervix.
HPV: Human Papilloma Virus, a group of viruses linked to cervical and other cancers.
Pap Test: Screening test for cervical cancer.
Colposcopy: Diagnostic procedure to examine the cervix for abnormalities.
ASCUS: Atypical squamous cells of undetermined significance.
LSIL: Low-grade squamous intraepithelial lesion.
Formulas & Equations
While there are no direct mathematical formulas for cervical cancer prevention, epidemiological rates and screening intervals are important:
Incidence Rate:
Screening Interval:
