 Back
BackTeaching and Learning Models for Health Behaviour Change
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Teaching and Learning Models in Health Behaviour Change
Introduction to Behaviour Change Theories
Understanding why individuals adopt or resist health-related behaviours is essential for effective patient education and health promotion. Several psychological models and theories help explain and predict health behaviour change, guiding nursing practice and patient education strategies.
Theories & Models of Health Behaviour Change
Overview of Key Models
Social Cognition Theories and Models: Focus on how people process information about health risks and benefits.
The Health Promotion Model: Emphasizes cognitive-perceptual and modifying factors influencing health actions.
Stage Models of Behaviour Change (Transtheoretical Model): Describe behaviour change as a process occurring in stages.
Social Cognitive Theory (SCT)
Core Concepts and Application
Social Cognitive Theory, developed by Albert Bandura, posits that behaviour is influenced by the dynamic interaction of personal factors, environmental influences, and behaviour itself. This model is widely used to understand health behaviour change.
Knowledge of Health Risks/Benefits: Awareness of the consequences of behaviours is foundational for change.
Perceived Self-Efficacy: The belief in one's ability to successfully perform a behaviour.
Outcome Expectations: Anticipated positive or negative results from changing behaviour.
Personal Health Goals: Setting specific, achievable objectives.
Facilitators and Impediments: Factors that help or hinder behaviour change.
Individual perception is crucial; people are more likely to change if they believe their current behaviour is harmful, believe change will help, and feel capable of making the change.
Self-Efficacy in SCT
Self-efficacy is a central predictor of behaviour change. It is the foundation of motivation and action, requiring both knowledge and a sense of control. Facilitators and impediments must be considered when planning interventions.
Sources of Self-Efficacy:
Past experiences (mastery)
Vicarious experiences (observing others)
Verbal persuasion (encouragement)
Physiological cues (emotional states)
The Health Belief Model (HBM)
Key Components and Application
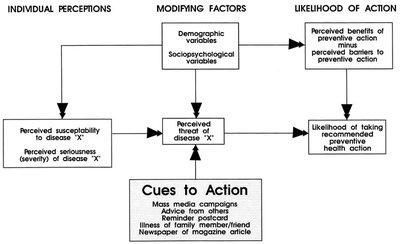
The Health Belief Model explains why some individuals take preventive health actions while others do not. It emphasizes the importance of individual perceptions, modifying factors, and cues to action.
Individual Perceptions: Perceived susceptibility and severity of a health issue.
Modifying Factors: Demographic and sociopsychological variables that influence perceptions.
Likelihood of Action: Determined by perceived benefits minus perceived barriers to action.
Cues to Action: Triggers such as media campaigns, advice, or reminders that prompt action.
Research suggests adding self-efficacy to the HBM, especially for complex behaviours like smoking cessation or safe sex practices.
Theory of Reasoned Action (TRA) and Theory of Planned Behaviour (TPB)
TRA: Predicting Behaviour from Intentions
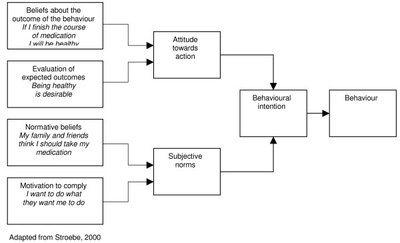
The Theory of Reasoned Action posits that a person's intention to perform a behaviour is the best predictor of that behaviour. Intentions are shaped by attitudes toward the behaviour and subjective norms (beliefs about others' expectations).
Attitude: Positive if the outcome is desirable, negative if undesirable.
Subjective Norms: Influence of significant others and motivation to comply with their expectations.
TPB: Adding Perceived Behavioural Control
The Theory of Planned Behaviour extends TRA by adding perceived behavioural control, which reflects the person's belief in their ability to perform the behaviour, considering opportunities and barriers.
Perceived Behavioural Control: Expectancy that the behaviour is within one's control, influenced by available resources and obstacles.
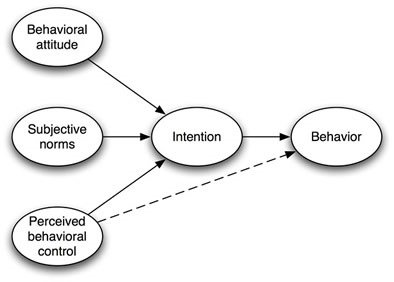
TPB is widely used in research on physical activity and other health behaviours.
Pender’s Health Promotion Model
Determinants of Health Behaviours
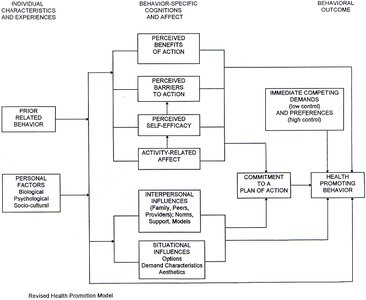
Pender’s Health Promotion Model focuses on factors that influence health-promoting behaviours, particularly in nursing practice. It considers individual characteristics, behaviour-specific cognitions, and behavioural outcomes.
Individual Characteristics and Experiences: Prior behaviour and personal factors (biological, psychological, sociocultural).
Behaviour-Specific Cognitions and Affect: Perceived benefits/barriers, self-efficacy, activity-related affect, interpersonal and situational influences, commitment to a plan of action, and competing demands/preferences.
Behavioural Outcome: Health-promoting behaviour as the end result.
Stage Models of Behaviour Change: The Transtheoretical Model
Stages and Processes of Change
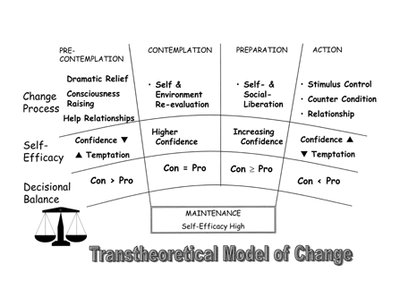
The Transtheoretical Model (TTM) describes behaviour change as a process that occurs in five stages. It emphasizes decision-making, self-efficacy, and the role of temptation in maintaining or relapsing from behaviour change.
Precontemplation: No intention to change behaviour.
Contemplation: Seriously considering change.
Preparation: Making small changes in readiness for action.
Action: Actively engaged in behaviour change.
Maintenance: Sustaining the new behaviour over time.
Key concepts include decisional balance (weighing pros and cons), self-efficacy, and temptation. Different processes of change are appropriate at different stages (e.g., consciousness raising, stimulus control).
Implications for Health Teaching
Effective Patient Education Strategies
Effective health teaching requires more than simply providing information. Nurses must consider factors influencing decision-making and involve clients in planning and goal setting. Providing understandable, reliable information and coaching clients to build new skills increases the likelihood of successful behaviour change.
Involve clients in planning and goal setting
Provide clear and reliable information
Coach clients in skill-building for mastery
