 Back
BackValvular Heart Disease: Pathophysiology, Diagnosis, and Treatment
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Valvular Heart Disease
Overview of Heart Valves
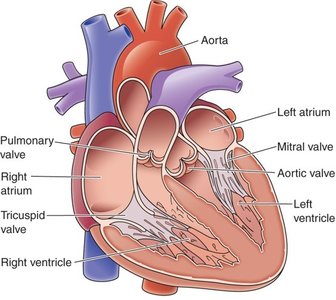
Heart valves are essential structures that ensure one-way blood flow through the heart. They are composed of leaflets made of endothelium-covered fibrous tissue. Damage or injury to these valves can disrupt normal blood flow, leading to a range of clinical consequences from mild symptoms to life-threatening conditions.
Valve Types:
Atrioventricular (AV) valves: Located between atria and ventricles; include the tricuspid (right) and mitral (left) valves.
Semi-lunar valves: Located between ventricles and main vessels; include the aortic and pulmonary valves.
Valve Function: Ensures unidirectional blood flow; prevents backflow.
Common Causes of Valve Disorders: Congenital defects, myocardial infarction (MI), trauma, infection, aging, arteriosclerosis, intravenous drug use.
Heart Sounds and Murmurs
Heart sounds are produced by the closure of heart valves and are important indicators of cardiac function. Abnormal sounds, known as murmurs, are caused by turbulent blood flow and may indicate underlying valvular disease.
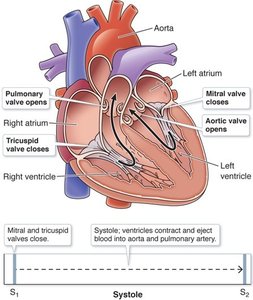
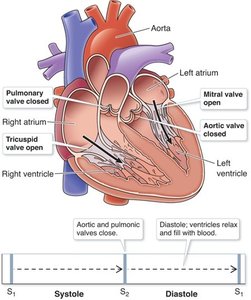
S1 ("lub"): Closure of AV valves at the beginning of systole.
S2 ("dub"): Closure of semi-lunar valves at the beginning of diastole.
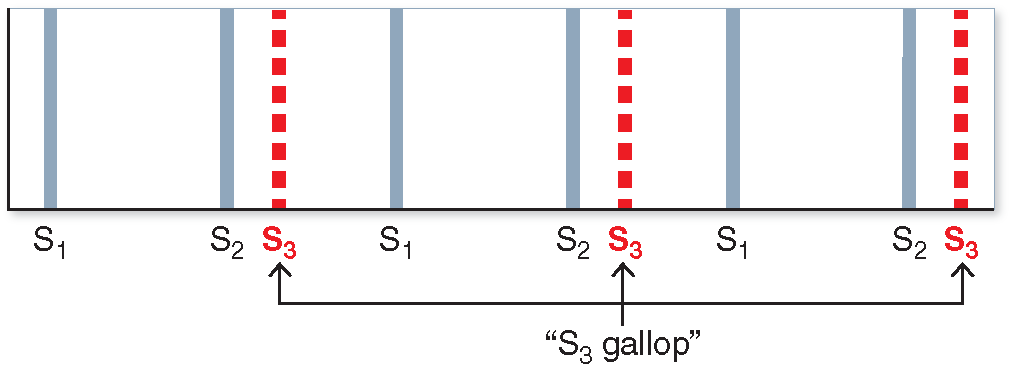
S3: Vibration of blood flow from atria to ventricles; normal in children and young adults, abnormal in older adults (S3 gallop).
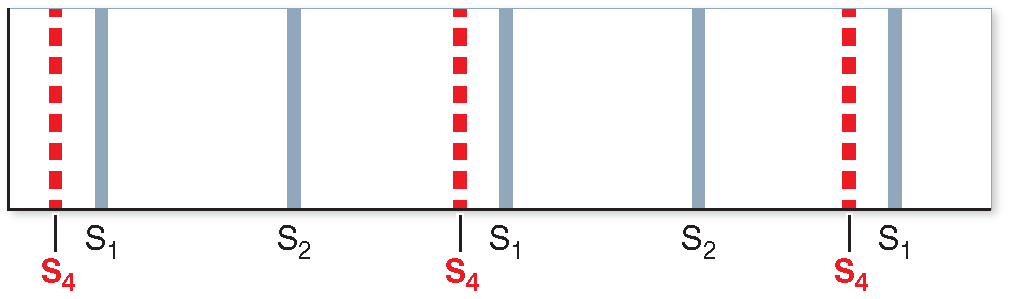
S4: Resistance to ventricular filling, often due to left ventricular hypertrophy (LVH).
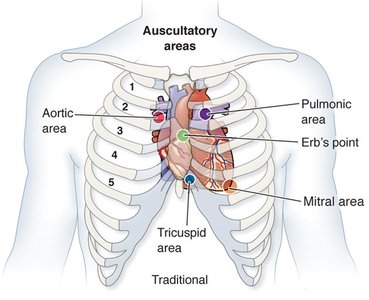
Cardiac Valve Auscultation
Auscultation is the process of listening to heart sounds using a stethoscope. Specific areas on the chest correspond to the location of each valve and are used to detect abnormal sounds.
Mitral: Apex of the heart, fifth intercostal space, midclavicular line.
Tricuspid: Left sternal border, fourth intercostal space.
Pulmonic: Second intercostal space, left sternal border.
Aortic: Second intercostal space, right sternal border.
Types of Heart Murmurs
Murmurs are classified as physiological (innocent) or pathological. Physiological murmurs occur during states of high blood flow and are usually asymptomatic. Pathological murmurs result from valve deformity or dysfunction and may require medical intervention.
Stenosis: Narrowed valve opening increases resistance to blood flow, leading to inefficient movement and increased cardiac workload.
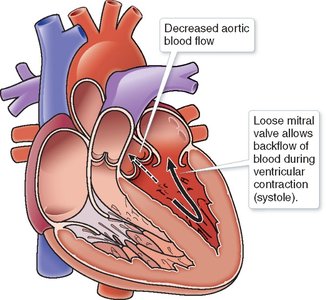
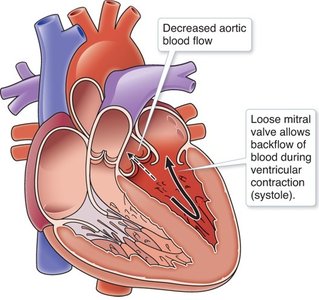
Regurgitation (Insufficiency): Loose valve allows backward leakage of blood, reducing forward ejection and causing volume overload.
Pathological Consequences of Valvular Disease
Valvular dysfunction can lead to several complications:
Dysrhythmias: Disruption of the cardiac conduction system due to chamber overstretching.
Thrombus Formation: Increased risk of clot due to turbulent and static blood flow.
Stroke: Elevated risk due to thrombus formation.
Myocardial Infarction (MI) and Heart Failure: Hypertrophy and ischemia of myocardium.
Assessment and Diagnosis
Diagnosis involves history, physical examination, and imaging studies:
History: Rheumatic fever, MI, myxomatous degeneration, arteriosclerotic calcification.
Physical Assessment: Inspection, palpation, auscultation for murmurs.
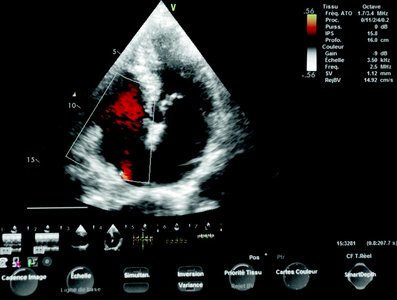
Imaging: Echocardiography (TTE, TEE, Doppler), cardiac CT, CMR, stress echocardiography, CCTA.
Clinical Description of Murmurs
Murmurs are described by grade (volume), timing (relation to S1/S2), location, radiation, pitch, quality, and shape.
Grade: 1 (faint) to 6 (loud).
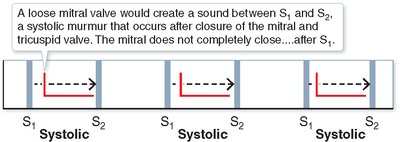
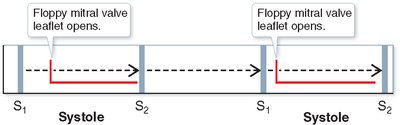
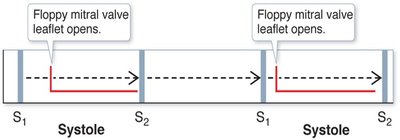
Timing: Systolic (S1 to S2), diastolic (S2 to S1), early, late, holosystolic.
Shape: Crescendo, decrescendo, plateau.


Treatment of Valvular Disease
Treatment options include medications and surgical interventions:
Medications: Nitrates, beta-blockers, anticoagulants, diuretics, antibiotics.
Surgical: Open heart surgery, transcatheter interventions, valve replacement (bioprosthetic or mechanical).
Valve Replacement Considerations: Patient age, comorbidities, bleeding risk, anticoagulation needs.
Specific Valve Disorders
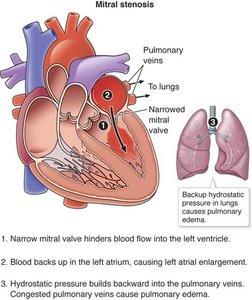
Mitral Stenosis
Mitral stenosis is often caused by rheumatic fever or mitral annular calcification. It leads to fluid backup in the left atrium and pulmonary edema.
Murmur: Diastolic, low-pitched rumble at heart apex.
Diagnosis: 3D Doppler echocardiogram, CCT, ECG, chest x-ray.
Treatment: Anticoagulants, diuretics, beta-blockers, prosthetic valve transplant, prophylactic antibiotics.
Mitral Insufficiency (Regurgitation)
Mitral insufficiency can be primary (anatomical abnormalities) or secondary (ischemia, papillary muscle dysfunction). It causes holosystolic murmur, decreased coronary flow, pulmonary symptoms, and atrial fibrillation.
Diagnosis: TTE, TEE, CMR, ECG, chest x-ray.
Treatment: Surgical repair preferred, MitraClip for transcatheter repair.
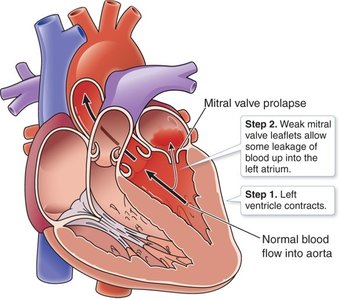
Mitral Valve Prolapse (MVP)
MVP is often asymptomatic but can be associated with Barlow's disease and ventricular arrhythmias. It is more common in females aged 14-30 years.
Murmur: Mid-systolic click followed by systolic murmur.
Treatment: Most do not require treatment; antibiotics not recommended for endocarditis prophylaxis.
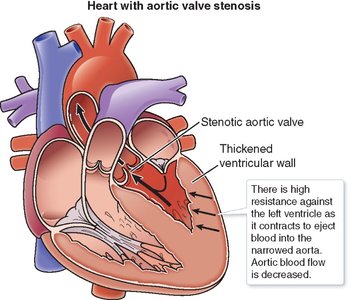
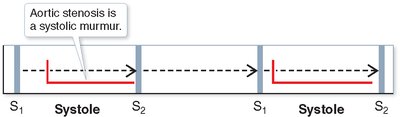
Aortic Stenosis
Aortic stenosis is caused by calcification, RHD, or congenital defects. It increases resistance for the left ventricle, leading to LVH and decreased aortic blood flow.
Murmur: Systolic, crescendo, low-pitched at second intercostal space.
Diagnosis: Echocardiography, CT-AVC, CMR, ECG, hsTnI, BNP.
Treatment: Valve replacement, bisphosphonates, medical management for asymptomatic patients.
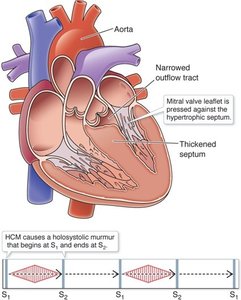
Hypertrophic Cardiomyopathy (HCM)
HCM is a genetic disorder characterized by asymmetric septal hypertrophy and LV outflow obstruction. It is a leading cause of sudden death in young individuals.
Murmur: Diamond-shaped systolic murmur.
Diagnosis: Echocardiography.
Treatment: Avoid strenuous exercise, beta-blockers, calcium channel blockers, surgical removal of excess tissue, septal ablation, valve replacement, pacemaker.
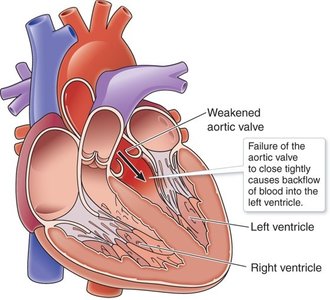
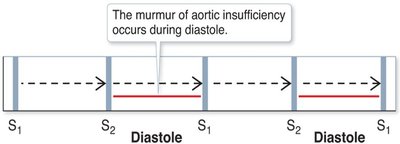
Aortic Insufficiency
Aortic insufficiency results from improper closure of the aortic valve, causing backflow into the left ventricle and pulmonary circulation.
Murmur: High-pitched, blowing, decrescendo diastolic murmur.
Diagnosis: TTE, TEE, color Doppler, CCT, CMR, ECG, chest x-ray.
Treatment: Valve replacement recommended; repair possible in some cases.
Pulmonic and Tricuspid Valve Disorders
Pulmonic and tricuspid valve disorders are less common. Pulmonic stenosis increases RV workload, while pulmonic insufficiency causes RV overload. Tricuspid stenosis and insufficiency lead to venous congestion and RV failure.
Pulmonic Stenosis: Harsh, systolic crescendo-decrescendo murmur; treated with balloon valvotomy or surgical replacement.
Pulmonic Insufficiency: Graham Steell murmur; treated with valve replacement.
Tricuspid Stenosis: Opening snap early in diastole; treated with valve replacement.
Tricuspid Insufficiency: Holosystolic murmur; treated by addressing underlying causes.
Clinical Concept Examples
Clinical Concept | Example |
|---|---|
Heart sounds | S3 sound: Commonly heard in heart failure; S4 sound: LVH due to HTN |
Prophylactic antibiotics | Valvular disorders before invasive treatment (e.g., dental work, IV catheter) |
MVP syndrome | Sporadic episodes of mitral leaflet prolapse, palpitations, dizziness, atypical chest pain |
IV drug use | Tricuspid valve abnormalities |
Alert!
Deformed or artificial valves are sites for bacterial growth, increasing the risk of infective endocarditis.
