 Back
BackGroup Psychotherapy: Principles, Theories, and Clinical Applications
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Group Psychotherapy
Definition
Group psychotherapy is a therapeutic modality in which a professionally trained leader organizes and guides a collection of individuals to work together toward achieving both individual and collective therapeutic goals. This approach leverages group dynamics to facilitate psychological growth and symptom relief.
History of Group Psychotherapy
Origins: Began in America in 1905 with Joseph H. Pratt, who led groups of tuberculosis patients at Massachusetts General Hospital.
Development: Samuel Slavson founded the American Group Psychotherapy Association in 1948, focusing on analytic group psychotherapy, especially with children.
European Influence: Jacob L. Moreno introduced role-playing and role-training methods in 1910, while Kurt Lewin developed field theory and the concept of group dynamics, emphasizing the group as more than the sum of its parts.
Systems Theory: Helen Durkin and Henrietta Glatzer integrated systems theory and psychodynamic principles, highlighting member-to-member interaction as central to therapeutic progress.
Principles and Theoretical Orientations
Major Theoretical Approaches
Psychodynamic: Focuses on unconscious processes, emotional attachments, and the resolution of past conflicts within the group context. Includes classic Freudian, object relations, and self-psychology perspectives.
Ego Psychology: Emphasizes defense mechanisms, adaptation, and the use of transference and countertransference within the group.
Interpersonal: Centers on "here and now" interactions, with Irvin Yalom's approach highlighting existential dilemmas and group cohesion.
Psychodrama: Uses dramatization and role-play to resolve personal issues, guided by a group leader (director).
Cognitive-Behavioral: Employs structured, manual-driven protocols based on learning theory, focusing on symptom relief and skill acquisition.
Systems-Oriented: Views the group as an entity with complex interactions, emphasizing roles and boundaries.
Transactional Analysis (TA): Developed by Eric Berne, TA replaces Freud's id-ego-superego with Parent, Adult, and Child ego states, aiming to change maladaptive "life scripts."
Self-Help Groups: Leaderless groups with shared issues (e.g., AA), providing social support and therapeutic benefit.
Comparison of Major Group Therapy Orientations
Orientation | Frequency (times/wk) | Screening | Group Size | Goals | Indications | Group Focus | Therapist Activity |
|---|---|---|---|---|---|---|---|
Supportive | 1–5 | Usually | 8–15 | Better adaptation to daily living | Crisis, severe emotional disorders | Here and now; environmental factors | Actively structures and leads group |
Psychodynamic | 1 or 2 | Always | 5–9 | Reconstruction of personality dynamics | Neuroses, mild personality disorders | Past and present; intragroup/extragroup dynamics | Active around interpretation |
Self-Help | 7 | Never | No limit | Social support | Shared life experiences | Education; emotional sharing | No formal leader |
Cognitive/Behavioral | 1–3 | Always | 5–10 | Relief of specific symptoms | Phobias, anxiety disorders | Training in symptom control methods | Very active in teaching skills |
Therapeutic Factors in Group Psychotherapy
Key Therapeutic Factors
Abreaction: Reliving repressed experiences with emotional release and insight.
Acceptance: Feeling accepted and tolerated by the group.
Altruism: Helping others and finding value in giving.
Catharsis: Emotional expression leading to relief.
Cohesion: Sense of unity and shared purpose; crucial for positive outcomes.
Consensual Validation: Reality confirmation through group comparison.
Contagion: Emotional expression in one member stimulates similar feelings in others.
Corrective Familial Experience: Group recreates family dynamics for psychological resolution.
Empathy: Understanding another's psychological perspective.
Identification & Imitation: Modeling behaviors after others, consciously or unconsciously.
Insight: Gaining awareness of maladaptive patterns (intellectual and emotional).
Inspiration: Installation of hope and optimism.
Interaction: Open exchange of ideas and feelings.
Interpretation: Leader helps members understand resistance and defenses.
Learning: Acquiring new knowledge and skills.
Reality Testing: Objective evaluation of self and others.
Transference: Projecting feelings onto the therapist or other members.
Universalization: Realizing one is not alone in their struggles.
Ventilation: Expressing suppressed feelings and secrets.
Theoretical Bases and Group Boundaries
Systems Theory and Group Boundaries
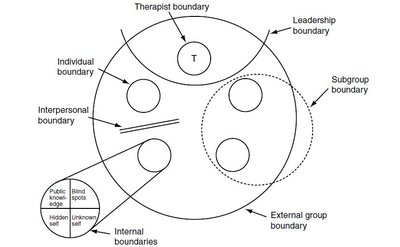
Group therapy is grounded in general systems theory, which posits that the group is more than the sum of its members. The group’s properties emerge from the dynamic interactions among members, with boundaries defining roles, relationships, and the flow of information.
Physical Boundaries: E.g., closing the door signals the start of a group.
Psychological Boundaries: Awareness of differences and transactions across boundaries (e.g., between leader and members, or among subgroups).
Types of Boundaries: Therapist, leadership, subgroup, individual, interpersonal, and internal member boundaries.
Pre-Group Preparation
Clarifying goals and purpose
Determining group composition
Defining the leader’s role
Setting rules for attendance, confidentiality, and fees
Arranging the therapy setting and time factors
Managing member loss/addition and extragroup socialization
Stages of Group Development
Five-Stage Model
Forming/Preaffiliation: Initial concerns about inclusion, acceptance, and group norms. Leader focuses on cohesion and goal compatibility.
Storming/Power and Control: Members test boundaries, negotiate differences, and experiment with self-disclosure. Leader mediates conflicts and maintains group focus.
Norming/Intimacy: Increased acceptance and mutuality. Members show individual differences and interact more spontaneously. Leader supports self-sufficiency but remains vigilant.
Performing/Differentiation: Mature group with deeper self-disclosure and interpersonal bonding. Members share responsibility; leader guides and prevents countertherapeutic detours.
Adjourning/Separation: Termination phase marked by feelings of loss, regression, and closure. Leader helps members process emotions and plan for life after the group.
Clinical Applications
Combined Individual and Group Therapy
Some conditions require both individual and group therapy ("combined therapy").
Potential issues include perceived favoritism and resistance to change, especially in personality disorders.
Combined therapy allows for integration of intrapsychic work and interpersonal experimentation.
Groups for Mood Disorders
Group therapy is effective for mood disorders, providing support, education, and skill-building.
Programs like the "life goals group" combine psychoeducation, cognitive-behavioral techniques, and self-management for bipolar disorder.
Groups for Personality Disorders
Interpersonal group psychotherapy and dialectical behavioral therapy (DBT) are effective for borderline personality disorder and related conditions.
DBT groups have been adapted for eating disorders, suicidal adolescents, and substance abuse.
Cognitive-behavioral group therapy (CBGT) is widely used for anxiety disorders, offering role modeling, peer feedback, and reinforcement.
Group Therapy with Patients With and Without Psychosis
Patients with Psychosis | Patients without Psychosis | |
|---|---|---|
Composition | Homogeneous for function | Homogeneous (brief); Heterogeneous (long-term) |
Functional Capacity | Poor ego strengths, interpersonal deficits | Can learn from feedback, empathy, altruism |
Goals | Crisis intervention, stabilization, social skills | Improved self-perception, interpersonal function, personality resolution |
Therapeutic Factors | Reality testing, identification, social support | Cohesion, challenging defenses, transference |
Leader Role | Active structuring, avoids aggressive themes | Catalyst for process, encourages confrontation |
Medication | Almost always included | May or may not be included |
Group Focus | Present and future | Here and now, historical focus |
Socialization | Encouraged | Discouraged |
Time Span | Brief and long-term | Brief (symptom focus), long-term (personality/behavior change) |
Participation | Involuntary and voluntary | Voluntary |
Research and Future Directions
Research Issues
Modern group psychotherapy is grounded in scientific research, with evidence supporting its efficacy.
Key factors for positive outcomes include pre-group selection, early structure, balance of individual and group factors, and active leadership.
Research tools are used to study group processes, leadership, and therapeutic mechanisms.
Future Directions
Trend toward eclectic, integrative group therapies with documentable, replicable interventions.
Increased use of cognitive, educational, and structured exercises, with greater patient responsibility for change.
