 Back
BackPhysical, Sensory, and Perceptual Development in Infancy CH. 4
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Physical, Sensory, and Perceptual Development in Infancy
Physical Changes in Infancy
Infancy is marked by rapid physical growth and significant changes in body structure and function. These changes lay the foundation for later development and are closely linked to brain maturation and environmental influences.
Growth Patterns: Infants grow 25–30 cm and triple their body weight in the first year. By age 2 (females) or 2.5 (males), toddlers are about half their adult height.
Head Proportion: Two-year-olds have proportionately larger heads to accommodate their nearly full-sized brains.
The Brain and the Nervous System
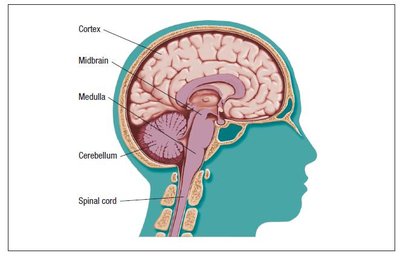
The brain undergoes dramatic development during the first two years, with different regions maturing at different rates.
Midbrain & Medulla: Regulate vital functions (heartbeat, respiration); most developed at birth.
Cortex: Least developed at birth; responsible for perception, movement, thinking, and language. Undergoes rapid growth postnatally.
Synaptogenesis & Pruning: Creation of synapses is followed by pruning, making the brain more efficient. Neuroplasticity allows for adaptation but also vulnerability to harm.
Myelinization: Myelin covers axons, improving nerve conductivity. Most rapid in the first two years, continuing into adolescence. The reticular formation (attention regulation) is not fully myelinated until the mid-20s.
Reflexes and Behavioural States
Newborns display a range of reflexes and behavioral states that reflect neurological development and adaptation to the environment.
Adaptive Reflexes: Essential for survival (e.g., sucking); some persist, others disappear in infancy or childhood.
Primitive Reflexes: Controlled by primitive brain regions; disappear by about 6 months.
Examples:
Rooting: Turning toward a cheek touch (disappears by 3 months).
Babinski: Toes fan out when foot is stroked (disappears by 12 months).
Moro: Startle response to noise or loss of support (disappears by 4–5 months).
States of Consciousness: Infants cycle through five states; sleep patterns stabilize with age. By 6 months, most sleep 13 hours/day with clear night and nap patterns.
Crying: Types include basic, anger, and pain cries. Colic involves intense, unexplained crying bouts.
Developing Body Systems and Motor Skills
Motor development is closely tied to changes in bones, muscles, and other body systems, following predictable patterns.
Cephalocaudal Pattern: Development proceeds from head downward.
Proximodistal Pattern: Development proceeds from the center outward.
Bones: Ossification (hardening) begins prenatally and continues through puberty, enabling motor development.
Muscles: Present at birth but initially small and watery; fat content declines by age 1.
Lungs & Heart: Improved efficiency and strength increase stamina by age 2.
Motor Skills:
Locomotor (gross motor): Crawling, walking.
Nonlocomotor: Head control, sitting.
Manipulative (fine motor): Grasping, using hands and fingers.
Developmental Milestones: Wide variability exists; cultural differences observed (e.g., Indigenous children may achieve gross motor skills earlier).
Gender Differences: Females may be ahead in manipulative skills; males are typically more active and show more rough-and-tumble play.
Table: Milestones of Motor Development in the First Two Years
Age (months) | Locomotor Skills | Non-locomotor Skills | Manipulative Skills |
|---|---|---|---|
1 | Stepping reflex | Lifts head slightly; follows moving objects with eyes | Holds object if placed in hand |
2–3 | Lifts head up to 90° when lying on stomach | Begins to swipe at objects | |
4–6 | Rolls over; sits with support; creeps | Holds head erect while sitting | Reaches for and grasps objects |
7–9 | Sits without support; crawls | Transfers objects between hands | |
10–12 | Pulls up, walks with support, then alone | Squats, stoops, plays patty cake | Shows hand preference; grasps spoon but poor aim |
13–18 | Walks backward, sideways; runs | Rolls ball; claps | Stacks two blocks; puts objects in/out of container |
19–24 | Walks up/down stairs, two feet per step | Jumps with both feet | Uses spoon; stacks 4–10 blocks |
Infant Health Promotion
Nutrition and health care are critical for optimal development in infancy. Malnutrition and illness can have lasting effects on growth and cognitive outcomes.
Breastfeeding: Superior to bottle-feeding; supports immune function and healthy gut microbiota.
Malnutrition:
Macronutrient malnutrition: Too few calories (marasmus) or too little protein (kwashiorkor) can cause severe developmental delays and mortality.
Micronutrient malnutrition: Vitamin/mineral deficiencies; Vitamin A supplementation can reduce mortality by 23%.
Health Care & Immunizations: Routine check-ups and immunizations are essential to prevent diseases such as measles, polio, and more.
Illness: Respiratory illnesses are common; chronic ear infections can lead to learning and language difficulties.
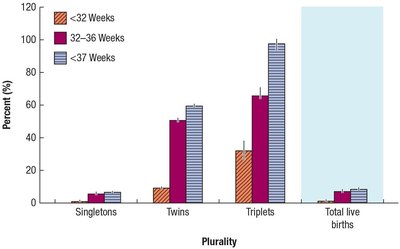
Preterm, Low-Birth-Weight, and Post-Term Infants
Birth timing and weight significantly affect early development and health outcomes.
Preterm: Born before 37 weeks; may lack adaptive reflexes and require special feeding. Developmental milestones are reached more slowly but often catch up by age 2–3.
Low-Birth-Weight (LBW): Less than 2.5 kg; most are preterm, but some are full-term. Progress is best compared using corrected age.
Post-Term: Born after 42 weeks; increased risk of mortality. Modern practices have reduced post-term deliveries.
Infant Mortality in Canada
Infant mortality rates have declined dramatically but remain higher in certain populations and under specific conditions.
Trends: From 134/1000 live births in 1901 to ~3.74/1000 in 2025.
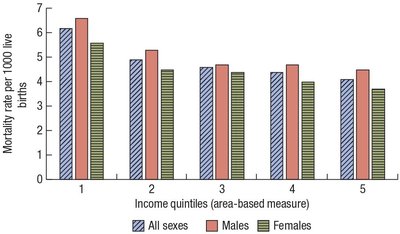
Disparities: Higher rates among lower-income, remote, and Indigenous populations.
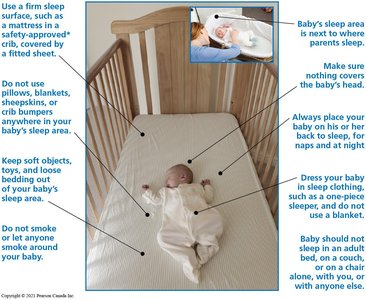
Sudden Unexpected Infant Death (SUID): Accounts for ~5% of infant deaths; most occur between 28 days and 1 year.
Safe Sleep Recommendations: Place infants on their backs, avoid soft bedding, and provide a smoke-free environment.
Sensory and Perceptual Development
Sensory Skills
Infants possess remarkable sensory abilities that develop rapidly in the first year, providing the foundation for perceptual and cognitive growth.
Vision: Newborns have poor visual acuity but can see near objects clearly. Vision improves rapidly, reaching near-adult levels by 6 months. Colour vision is present by 1 month.
Tracking: Ability to follow moving objects develops quickly.
Hearing: Nearly adult-like at birth; infants can locate sounds and discriminate speech sounds.
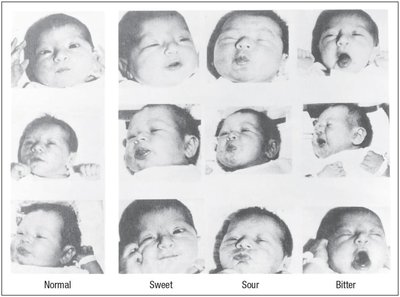
Smell & Taste: Well developed; infants react differently to basic tastes and can recognize their mother's scent.
Touch & Motion: Most developed sense at birth; essential for emotional bonding and brain development.
Perceptual Skills
Perceptual development involves the interpretation of sensory information, allowing infants to make sense of their environment.
Research Methods:
Preference Technique: Measures looking time to assess interest.
Habituation/Dishabituation: Measures response to new stimuli after repeated exposure.
Operant Conditioning: Assesses learned responses to changes in stimuli.
Critical Periods: Specific times when sensory input is necessary for normal development (e.g., vision).
Depth Perception: Develops through binocular, monocular, and kinetic cues between 3–7 months.
Looking Patterns: Infants initially focus on contrast and motion, then scan entire objects and patterns by 2–4 months.
Face Perception: Infants prefer attractive faces and their mother's face; reciprocal eye gaze emerges by 6 months.


Listening and Speech Perception
Infants are highly sensitive to speech sounds and can discriminate between syllables and voices from an early age.
Speech Sound Discrimination: At 1 month, infants distinguish syllables (e.g., pa vs. ba); at 6 months, they distinguish word patterns. This ability narrows to native language sounds by the end of the first year.
Voice Recognition: Newborns prefer and recognize their mother's voice, a skill learned in utero.
Other Sound Patterns: By 6 months, infants recognize melodies and non-speech sound patterns.
Intermodal Perception
Infants can integrate information from multiple senses to form unified perceptions, a skill that emerges early and becomes common by 6 months.
Cross-Modal Transfer: Ability to transfer information from one sense to another (e.g., recognizing an object by touch and then by sight).
Theories of Perceptual Development
Debate exists between nativist (innate abilities) and empiricist (experience-dependent) perspectives. Most evidence supports an integration of both: infants are born with impressive sensory capacities, but experience is essential for normal development.
Nativism: Sensory abilities are largely innate.
Empiricism: Experience and exposure are necessary for full development.
Integration: Both nature and nurture contribute to perceptual development.
