 Back
BackPsychological Disorders II: Anxiety, Obsessive-Compulsive, Depressive Disorders, and Schizophrenia
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Anxiety, Obsessive-Compulsive, & Depressive Disorders
Anxiety Disorders
Anxiety disorders are characterized by excessive, irrational, and maladaptive fear or nervousness. These disorders are common and often occur alongside other mental health conditions (comorbidity). Symptoms often include physiological responses such as fight-or-flight, freezing, or fainting.
Generalized Anxiety Disorder (GAD): Persistent and elevated anxiety levels, often in response to everyday life stressors. Individuals experience a general sense of unease that is difficult to control. The amygdala is particularly sensitive to stressors in GAD.
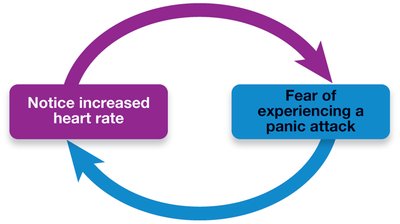
Panic Disorder: Characterized by sudden, intense episodes of fear known as panic attacks. These can occur unexpectedly and may lead to avoidance behaviors.
Agoraphobia: Intense fear of having a panic attack in public places, leading to avoidance of such situations.
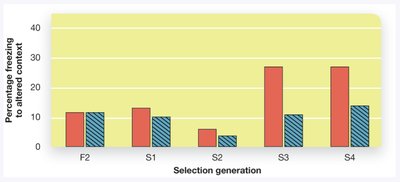
Specific Phobia: Intense fear of a particular object, activity, or organism. Genetic factors may contribute, as shown by selective breeding studies of fear responses.
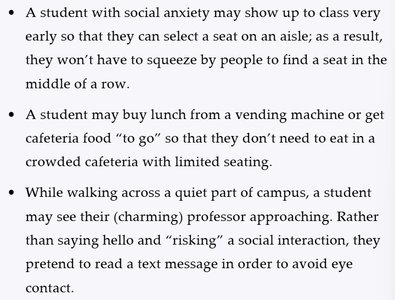
Social Phobia (Social Anxiety Disorder): Strong fear of being judged or embarrassed in social situations. Cultural variants such as Hikikomori (extreme social withdrawal) are also noted.
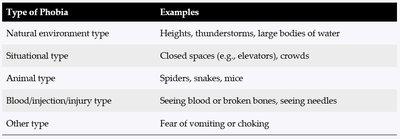
Type of Phobia | Examples |
|---|---|
Natural environment type | Heights, thunderstorms, large bodies of water |
Situational type | Closed spaces (e.g., elevators), crowds |
Animal type | Spiders, snakes, mice |
Blood/injection/injury type | Seeing blood or broken bones, seeing needles |
Other type | Fear of vomiting or choking |
Example: A student with social anxiety may avoid crowded cafeterias or eye contact with professors to reduce anxiety.
Additional info: Anxiety disorders are often treated with cognitive-behavioral therapy (CBT) and, in some cases, medication such as SSRIs or benzodiazepines.
Obsessive-Compulsive Disorder (OCD)
OCD is marked by persistent, unwanted thoughts (obsessions) and repetitive, ritualistic behaviors (compulsions) performed to reduce anxiety. Common obsessions include fears of contamination, while compulsions may involve excessive cleaning or checking.
Obsessions: Intrusive thoughts that cause distress (e.g., fear of germs).
Compulsions: Ritualistic behaviors aimed at controlling obsessions (e.g., handwashing).
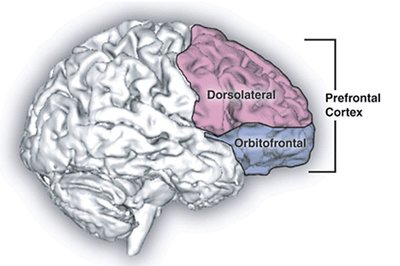
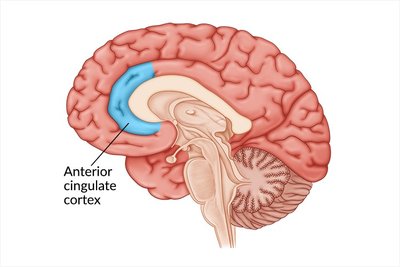
Neural Circuitry: The orbitofrontal cortex (OFC), basal ganglia, and thalamus form a loop implicated in OCD. The dorsolateral prefrontal cortex (DLPFC) and anterior cingulate cortex (ACC) are also involved in cognitive control and error detection.
Example: The "Lady Macbeth effect" refers to the urge to cleanse oneself after moral transgressions, illustrating the link between obsessions and compulsions.
Additional info: OCD is often treated with exposure and response prevention (ERP) therapy and SSRIs.
Mood Disorders
Mood disorders involve disturbances in emotional state, ranging from prolonged sadness to extreme mood swings. Major depressive disorder (MDD) and bipolar disorder are the primary mood disorders discussed.
Major Depressive Disorder (MDD): Characterized by persistent sadness, hopelessness, social withdrawal, and cognitive/physical sluggishness. A pessimistic explanatory style (internalizing, stabilizing, globalizing) is common.
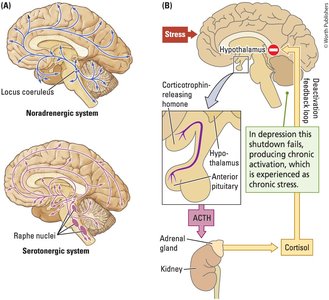
Biological Factors: Overactivity of the amygdala and hypothalamic-pituitary-adrenal (HPA) axis increases stress hormones (e.g., cortisol). The hippocampus (HC) and frontal cortex (FC) inhibit this response, but reduced neurogenesis in the HC is observed in depression. The nucleus accumbens is linked to anhedonia (loss of pleasure), and the medial prefrontal cortex (mPFC) is associated with rumination.
Neurochemistry: Serotonin (5-HT) deficits are implicated; selective serotonin reuptake inhibitors (SSRIs) are common treatments.
Bipolar Disorder: Involves alternating episodes of mania (elevated mood, energy) and depression. Treatment is challenging due to the severity and variability of symptoms.
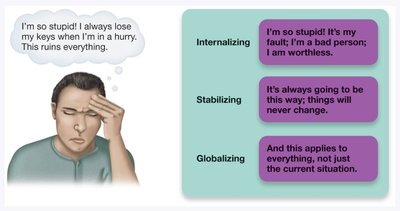
Example: A person with MDD may interpret losing their keys as a sign of personal failure, expecting it to always happen and generalizing it to all aspects of life.
Additional info: Cognitive-behavioral therapy and pharmacological interventions are standard treatments for mood disorders.
Schizophrenia
Symptoms and Phases
Schizophrenia is a severe brain disorder characterized by significant breaks from reality, disorganized thinking, and emotional disturbances. It is distinct from dissociative identity disorder (DID).
Phases:
Prodromal: Negative symptoms such as social withdrawal and catatonia.
Active: Positive symptoms including hallucinations (false perceptions) and delusions (false beliefs, e.g., paranoia, grandeur), as well as disorganized behavior.
Residual: Ongoing symptoms after acute episodes.
Subtypes: Paranoid, disorganized, and catatonic schizophrenia.

Example: Auditory hallucinations, such as hearing voices, are a common positive symptom.
Explanations and Causes
Multiple factors contribute to the development of schizophrenia, including genetics, brain structure, neurochemistry, and environmental influences.
Genetics: Family and twin studies show a strong genetic component. The risk increases with genetic closeness to an affected individual.
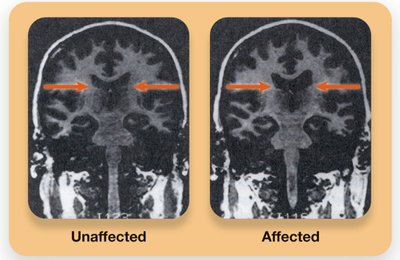
Brain Differences: Enlarged ventricles, reduced frontal cortex activity, increased dopamine (DA) activity (positive symptoms), and underactive glutamate (GLU) systems (negative symptoms).
Neurodevelopmental Hypothesis: Prenatal factors (maternal stress, malnutrition, winter birth) and adolescent factors (excessive synaptic pruning in the prefrontal cortex) increase risk.
Environmental Stressors: Urban living, low social support, high emotional expressiveness (EE), and cannabis use are associated with increased risk.
Example: The prodromal phase may begin in adolescence, with symptoms worsening into adulthood.
Additional info: Antipsychotic medications and psychosocial interventions are primary treatments for schizophrenia.
References and Resources
York mental health resources: Student Counselling, Health & Well-being
Good2Talk helpline
Further reading: Hikikomori, Lady Macbeth effect, Catatonia
