 Back
BackSchizophrenia Spectrum, Psychotic Disorders, and Substance-Related/Addictive Disorders
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Schizophrenia Spectrum and Other Psychotic Disorders
Overview of Schizophrenia
Schizophrenia is a chronic psychotic disorder marked by episodes of a break with reality, including delusions, hallucinations, disorganized thinking, incoherent speech, and bizarre behavior. It is a major mental health condition with significant personal and societal impacts.
Delusions: False beliefs not based in reality (e.g., persecution, grandeur, reference, being controlled).
Hallucinations: Sensory perceptions without external stimuli (most commonly auditory).
Disorganized Speech: Includes neologisms, perseveration, clanging, and blocking.
Grossly Disorganized or Catatonic Behavior: Includes catatonia, odd gestures, waxy flexibility, and stupor.
Positive Symptoms: Excesses such as hallucinations, delusions, and disorganized behavior.
Negative Symptoms: Deficits such as social withdrawal, flattened affect, alogia, anhedonia, and avolition.
Historical Conceptions and Clinical Features
Emil Kraepelin: Described 'dementia praecox' as an early form of schizophrenia.
Eugen Bleuler: Coined the term 'schizophrenia' and identified the 'Four As': abnormal associations, autistic behavior/thinking, abnormal affect, and ambivalence.
Kurt Schneider: Distinguished between first-rank (core) and second-rank (non-specific) symptoms.
Prevalence and Impact
About 1% of adults are affected at some point.
High rates of unemployment, substance abuse, and suicide attempts.
Stigma and misconceptions about violence are common.
Onset typically in late teens or early 20s; men are at slightly higher risk.
Phases of Schizophrenia
Prodromal Phase: Early signs and decline in functioning before the first acute episode.
Acute (Active) Phase: Full psychotic symptoms emerge.
Residual Phase: Symptoms subside but some impairment remains.
Theoretical Perspectives
Multiple perspectives attempt to explain the development and maintenance of schizophrenia.
Psychodynamic: Overwhelming of the ego by primitive impulses; regression to early developmental stages.
Learning: Lack of social reinforcement and increased attention to inner fantasy world; modeling of bizarre behavior.
Biological: Genetic predisposition, dopamine hypothesis, brain abnormalities, prenatal factors (e.g., vitamin D deficiency).
Family Theories: Schizophrenogenic mother, double-bind communication, communication deviance, and expressed emotion.
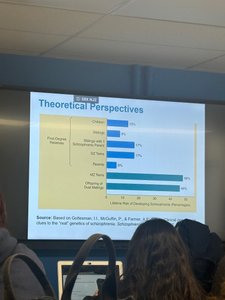
Image 1: Bar graph showing the relative support for different theoretical perspectives on schizophrenia, including genetic, family, and environmental factors.
Diathesis-Stress Model
The diathesis-stress model posits that schizophrenia results from the interaction of genetic vulnerability (diathesis) and environmental stressors.
Diathesis: Genetic or biological predisposition.
Stress: Environmental factors such as family conflict, trauma, or substance use.
Protective Factors: Supportive family, coping skills, and early intervention can reduce risk.
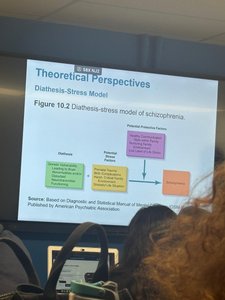
Image 2: Diagram illustrating how genetic vulnerability and environmental stressors interact to produce schizophrenia.
Other Psychotic Disorders
Delusional Disorder: Persistent non-bizarre delusions without other major symptoms.
Schizoaffective Disorder: Features of both schizophrenia and mood disorders.
Schizophreniform Disorder: Schizophrenia-like symptoms lasting 1-6 months.
Brief Psychotic Disorder: Sudden onset of psychosis lasting more than one day but less than one month, often after trauma.
Treatment Approaches
Biological: Antipsychotic drugs (typical and atypical), with risks of extrapyramidal symptoms (e.g., tardive dyskinesia, parkinsonism).
Psychosocial: Learning-based therapies (reinforcement, token economy), social skills training, cognitive-behavioral therapy (CBT), family intervention, and community support.
Comprehensive Care: Canadian guidelines recommend a combination of medication, psychoeducation, crisis intervention, and housing support.
Substance-Related and Addictive Disorders
Overview and Classification
Substance-related and addictive disorders involve maladaptive patterns of substance use leading to significant impairment or distress. These include both substance use disorders and behavioral addictions.
Polydrug Use: Use of multiple substances simultaneously.
Psychoactive Substances: Chemicals that alter mood, perception, or brain function.
Intoxication: State of behavioral or psychological change due to recent substance use.
Withdrawal Syndrome: Symptoms following reduction or cessation of substance use after dependence has developed.
Image 3: Slide summarizing withdrawal syndromes, including symptoms such as dryness in the mouth, nausea, vomiting, weakness, tachycardia, anxiety, depression, hallucinations, and more.
Key Concepts
Addiction: Impaired control over substance use, often with physiological dependence.
Physiological Dependence: Body adapts to the substance, leading to tolerance and withdrawal symptoms.
Psychological Dependence: Emotional or mental reliance on a substance, even without physical dependence.
Pathways to Substance Use Disorder
Experimentation → Routine Use → Addiction/Dependence
Types of Substances
Depressants: Lower CNS activity (e.g., alcohol, opiates). Risks include overdose, addiction, and health complications.
Opiates: Strongly addictive, provide euphoria and pain relief (e.g., morphine, heroin, codeine, fentanyl).
Stimulants: Increase CNS activity (e.g., amphetamines, cocaine). Can cause euphoria, increased heart rate, and risk of addiction.
Hallucinogens: Cause sensory distortions (e.g., LSD, psilocybin, mescaline, marijuana).
Psychological and Sociocultural Perspectives
Learning: Operant conditioning, negative reinforcement, and observational learning contribute to substance use.
Cognitive: Beliefs and expectations about drug effects influence use (e.g., placebo effects, alcohol myopia).
Psychodynamic: Substance abuse as a sign of oral fixation or unresolved conflicts.
Sociocultural: Cultural norms, peer pressure, and social environment play a role.
Treatment Approaches
Biological: Detoxification under medical supervision, medication-assisted treatment.
Support Groups: Alcoholics Anonymous (AA), Al-Anon, and other peer support networks.
Residential Programs: Hospital or therapeutic residence for severe cases.
Cognitive-Behavioral: Self-control strategies, social skills training, cue-exposure, and relapse-prevention training.
Table: Major Types of Substances and Their Effects
Substance Type | Main Effects | Examples |
|---|---|---|
Depressants | Reduce CNS activity, induce relaxation, impair cognition | Alcohol, benzodiazepines, opiates |
Stimulants | Increase CNS activity, elevate mood, increase alertness | Amphetamines, cocaine, caffeine |
Hallucinogens | Distort perception, induce hallucinations | LSD, psilocybin, marijuana |
