 Back
BackBlood Physiology: Blood Types, Immune Reactions, and Disorders
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Blood Physiology
Cauterization of a Nosebleed with Silver Nitrate
Cauterization is a chemical method used to stop persistent anterior nosebleeds (epistaxis) when other measures such as pressure, ice, or nasal packing fail. Silver nitrate is applied to visible bleeding vessels on the anterior nasal septum, causing a chemical burn that leads to coagulative necrosis of mucosal tissue.
Chemical Reaction: Silver nitrate reacts with tissue proteins to form an Ag-protein complex and nitric acid.
Equation:
Silver ions (Ag+) precipitate tissue proteins, forming a barrier and are reduced to metallic silver (Ag0).
Nitric acid (HNO3) contributes to local tissue destruction, aiding coagulation.
Blood Types and Transfusion Compatibility
ABO and Rh Blood Group Systems
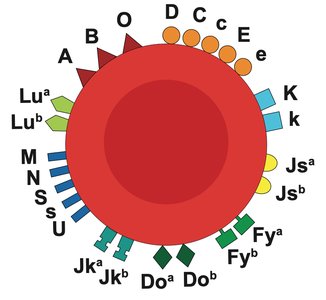
Blood types are determined by the presence or absence of specific antigens on the surface of red blood cells (RBCs). The two main systems are the ABO system and the Rh factor.
ABO System: Types A, B, AB, and O refer to different surface antigens.
Rh System: Presence (Rh+) or absence (Rh−) of the D antigen.
Example: A+ blood has A antigens and the Rh antigen; B− has B antigens but no Rh antigen.
Antigens and Antibodies
Antigens are found on the surface of RBCs and act as cell ID tags, determining blood type. Antibodies are found in blood plasma and target foreign antigens.
Innate ABO Antibodies: Individuals are born with antibodies against A or B antigens they do not possess.
Type A: Has A antigens, anti-B antibodies.
Type B: Has B antigens, anti-A antibodies.
Type O: No antigens, both anti-A and anti-B antibodies.
Type AB: Both antigens, no ABO antibodies.
Transfusion Reactions
If mismatched blood is transfused, an immediate immune response (hemolytic reaction) occurs, destroying the donor RBCs. Symptoms can include fever, chills, back pain, hemoglobinuria, shortness of breath, hypotension, chest pain, nausea, vomiting, and jaundice.
Symptom | Cause |
|---|---|
Fever and chills | Immune response to foreign blood cells |
Back or flank pain | Kidney stress due to filtering damaged red cells |
Dark/red urine | Free hemoglobin from destroyed RBCs excreted by kidneys |
Shortness of breath | Reduced oxygen-carrying capacity |
Low blood pressure | Immune activation and systemic inflammation |
Chest pain | Reduced oxygenation and stress on the heart |
Nausea and vomiting | Systemic inflammatory response |
Jaundice (delayed) | Breakdown of RBCs releasing bilirubin |

Complications of Untreated Hemolytic Reactions
Acute kidney injury from hemoglobin buildup
Shock from widespread immune response
Disseminated intravascular coagulation (DIC): widespread clotting followed by bleeding
Death in severe, untreated cases
Diagnosis and Prevention
Immediate cessation of transfusion
Blood tests (e.g., direct antiglobulin) to confirm immune hemolysis
Urine test for free hemoglobin
Prevention: Careful blood type matching is essential.

Rh System: Acquired Antibodies and Rh Incompatibility
Unlike the ABO system, individuals are not born with anti-Rh antibodies. Rh-negative individuals can develop anti-Rh antibodies after exposure to Rh-positive blood (e.g., pregnancy, transfusion). Once sensitized, the immune system can attack Rh-positive blood in the future.
Rh reactions may develop over time after sensitization, especially dangerous in pregnancy or repeat transfusions.
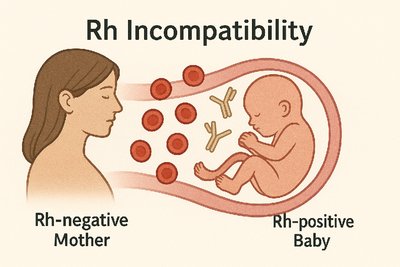
Rh Incompatibility in Pregnancy
Rh incompatibility occurs when an Rh-negative mother carries an Rh-positive fetus. The mother's immune system may produce antibodies against fetal RBCs, which can cross the placenta and attack the baby's RBCs, leading to hemolytic disease of the newborn (HDN) or erythroblastosis fetalis.
Usually not a problem in the first pregnancy, but risk increases with subsequent Rh-positive pregnancies if sensitization has occurred.
Mild cases: Anemia, jaundice
Severe cases: Heart failure, brain damage, stillbirth
Prevention with RhoGAM
RhoGAM is an injection given to Rh-negative mothers around 28 weeks of pregnancy and within 72 hours after delivery if the baby is Rh-positive, or after any bleeding, miscarriage, or invasive procedures.
It prevents the mother's immune system from producing anti-Rh antibodies.
Blood type tests early in pregnancy identify risk; if both parents are Rh-negative, there is no risk.
Management if Sensitization Occurs
Step | Goal |
|---|---|
Monitor antibody levels | Assess risk to fetus |
Ultrasound & Doppler | Detect fetal anemia |
Intrauterine transfusion | Treat anemia in womb |
Early delivery | Prevent worsening damage |
NICU care | Support after birth |
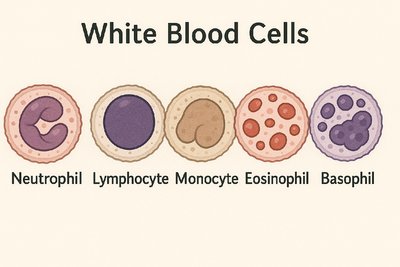
White Blood Cells (WBCs) and Immune Function
Types of White Blood Cells
White blood cells are part of the immune system, produced in bone marrow and found in blood and lymphatic tissue. They are classified as granulocytes or agranulocytes based on the presence of cytoplasmic granules.
Group | Cell Types | Key Feature |
|---|---|---|
Granulocytes | Neutrophils, Eosinophils, Basophils | Visible granules in cytoplasm |
Agranulocytes | Lymphocytes, Monocytes | Lack visible granules |
Cell Type | Function | Nucleus | Granules? | Size (µm) |
|---|---|---|---|---|
Neutrophils | Phagocytose bacteria | Multi-lobed | Yes (fine) | 12–15 |
Eosinophils | Fight parasites, allergies | Bi-lobed | Yes (red) | 12–17 |
Basophils | Release histamine | Obscured | Yes (dark) | 12–15 |
Lymphocytes | Antibody & T-cell immunity | Large, round | No | 7–10 (small), 10–15 (large) |
Monocytes | Phagocytosis, become macrophages | Kidney-shaped | No | 15–20 |
Disorders of the Blood and Immune System
Mononucleosis
Viral infection, most commonly caused by Epstein-Barr virus (EBV)
Spread mainly through saliva
Common in teens and young adults
CBC may show elevated lymphocytes and atypical lymphocytes
Sickle Cell Disease
Hereditary blood disorder caused by a mutation in the HBB gene affecting hemoglobin (HbS)
RBCs become sickle-shaped, rigid, and sticky, leading to anemia and vessel blockage
Inheritance: Two copies of the gene cause disease; one copy = carrier (trait)
Eosinophilia
Elevated eosinophil count (>500 cells/µL)
Causes include parasitic/fungal infections, allergies, drug reactions, hematologic malignancies, autoimmune diseases, and adrenal insufficiency
Eosinophilia is a sign, not a disease; identifying the cause is critical
Anemia
Anemia is a condition where the blood lacks enough healthy RBCs or hemoglobin, leading to reduced oxygen delivery to tissues. It is a sign of underlying disease, not a disease itself.
Normal hemoglobin levels: Men 13.5–17.5 g/dL, Women 12.0–15.5 g/dL
Type | Cause | RBC Appearance |
|---|---|---|
Iron-deficiency | Poor diet, blood loss | Small (microcytic), pale |
Vitamin B12/Folate | Malabsorption, poor intake | Large (macrocytic) |
Hemolytic | RBC destruction (e.g., autoimmune, sickle cell) | Normal or varied |
Aplastic | Bone marrow failure | Low count of all cells |
Blood Clotting and Cardiovascular Risk
Blood Clots (Thrombi)
A blood clot is a clump of blood that has changed from liquid to a gel-like state, part of the body's natural response to stop bleeding (hemostasis). Beneficial clotting involves vascular spasm, platelet plug formation, and coagulation.
Platelets, clotting factors, and fibrin are essential for clot formation.
LDL Cholesterol and Clot Risk
LDL (low-density lipoprotein) is known as "bad cholesterol" because high levels can lead to plaque formation in arteries (atherosclerosis). Plaques can rupture, triggering clot formation inside arteries, which may result in myocardial infarction (heart attack) or stroke.
Feature | Fibrous Plaque | Complicated Plaque |
|---|---|---|
Structure | Stable core of lipids, thick fibrous cap | Ruptured/eroded cap, exposed core |
Stability | More stable, less likely to rupture | Unstable, high risk of rupture |
LDL Role | Accumulated but contained | Core filled with oxidized LDL, inflammatory cells |
Inflammation | Low to moderate | High |
Thrombosis Risk | Low | High |
Clinical Impact | Gradual narrowing of arteries | Sudden blockage → heart attack or stroke |
Harmful Clotting (Thrombosis)
Clots can form inside blood vessels, leading to heart attack (coronary thrombosis), stroke (cerebral thrombosis), or deep vein thrombosis (DVT) which can cause pulmonary embolism.
Summary Table: White Blood Cell Types and Functions
Cell Type | Size (µm) | % of WBCs | Function | Nucleus | Granules |
|---|---|---|---|---|---|
Neutrophils | 12–15 | 60–70% | Phagocytose bacteria | Multi-lobed | Pale, fine |
Eosinophils | 12–17 | 1–4% | Combat parasites, allergies | Bi-lobed | Red |
Basophils | 12–15 | <1% | Release histamine | Obscured | Dark |
Lymphocytes | 7–10 (small), 10–15 (large) | 20–25% | Produce antibodies, kill infected cells | Large, round | None |
Monocytes | 15–20 | 3–8% | Phagocytosis, become macrophages | Kidney-shaped | None |
