 Back
BackBlood: Structure, Function, and Disorders (Chapter 17 Study Guide)
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Blood: Structure, Function, and Disorders
Functions of Blood
Blood is a vital connective tissue responsible for transport, regulation, and protection within the human body.
Transport: Delivers oxygen and nutrients to cells, removes metabolic wastes, and transports hormones.
Regulation: Maintains body temperature, pH balance (using buffers and bicarbonate ions), and fluid volume.
Protection: Prevents blood loss (hemostasis) and infection (via antibodies, complement proteins, and white blood cells).
Physical Characteristics and Volume
Blood is a sticky, opaque fluid with a metallic taste. Its color varies with oxygen content: scarlet red when oxygenated, dark red when deoxygenated. The pH is slightly basic (7.35–7.45), and average volume is 5–6 L in males and 4–5 L in females.
Composition of Blood
Blood Components
Blood is the only fluid tissue in the body, classified as connective tissue. It consists of a liquid matrix called plasma and formed elements (cells or cell fragments suspended in plasma): erythrocytes (RBCs), leukocytes (WBCs), and platelets.
Plasma: Straw-colored, sticky fluid; 90% water, contains over 100 dissolved solutes (nutrients, gases, hormones, wastes, proteins, inorganic ions).
Plasma Proteins: Most abundant solutes, produced mainly by the liver. Albumin (60% of plasma proteins) functions as a carrier, blood buffer, and maintains osmotic pressure.
Formed Elements
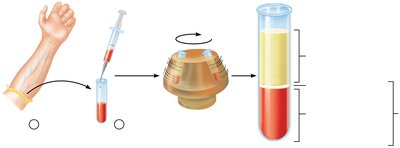
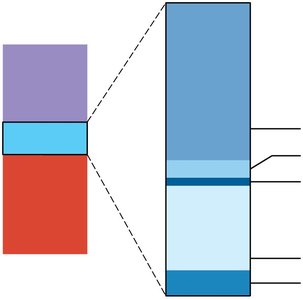
Spinning blood in a centrifuge yields three layers:
Erythrocytes (RBCs): Bottom layer (~45% of whole blood, measured as hematocrit).
Buffy coat: Middle layer (<1%), contains WBCs and platelets.
Plasma: Top layer (~55%).
Erythrocytes (Red Blood Cells)
Structural Characteristics
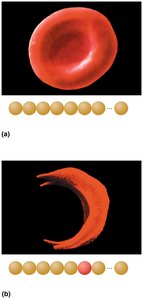
Erythrocytes are small (7.5 μm diameter), biconcave, anucleate cells specialized for gas transport. Their shape increases surface area for gas exchange, and they lack mitochondria, relying on anaerobic glycolysis for energy.
Biconcave shape: Maximizes surface area for gas exchange.
Filled with hemoglobin: 97% of cell volume (excluding water).
Flexible membrane: Contains spectrin protein for shape change.

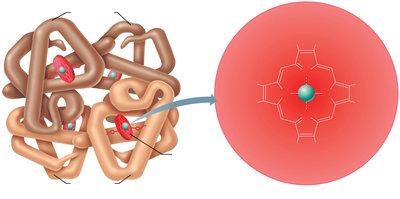
Hemoglobin Structure and Function
Hemoglobin is the oxygen-carrying protein in RBCs, composed of four globin chains (two alpha, two beta) and four heme groups. Each heme contains an iron atom that binds oxygen reversibly.
Oxygen transport: Each hemoglobin molecule can carry four O2 molecules.
CO2 transport: 20% of CO2 binds to hemoglobin as carbaminohemoglobin.
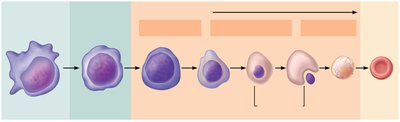
Production of Erythrocytes (Erythropoiesis)
Erythropoiesis is the process of RBC formation, occurring in red bone marrow. It involves several stages, from hematopoietic stem cells to mature erythrocytes.
Hematopoietic stem cell (hemocytoblast): Source of all blood cells.
Committed cell: Can only become RBCs.
Reticulocyte: Immature RBC with ribosomes; increases after blood loss.
Mature erythrocyte: Anucleate, cannot divide.
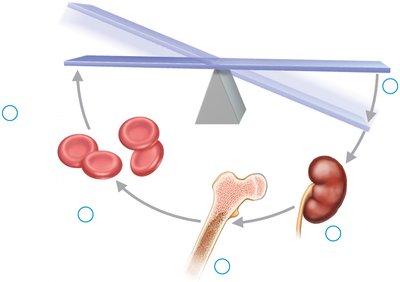
Regulation of Erythropoiesis
RBC production is regulated by erythropoietin (EPO), a hormone released by the kidneys in response to hypoxia (low oxygen levels). Balance is maintained by hormonal control and dietary requirements (amino acids, iron, vitamin B12, folic acid).
Too few RBCs: Tissue hypoxia.
Too many RBCs: Increased blood viscosity.
EPO: Stimulates RBC production; enhanced by testosterone.
Life Cycle and Fate of Erythrocytes
RBCs have a lifespan of 100–120 days. Old RBCs are trapped and broken down in the spleen, liver, and bone marrow. Hemoglobin is degraded: iron is stored or reused, heme is converted to bilirubin (excreted in bile), and globin is broken down to amino acids.

Erythrocyte Disorders
Anemia
Anemia is a condition of low RBC count or low hemoglobin, resulting in reduced oxygen-carrying capacity. It is classified by cause: blood loss, insufficient RBC production, or excessive RBC destruction.
Blood loss: Hemorrhagic anemia (acute or chronic).
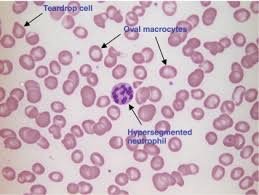
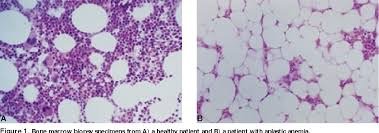
Insufficient production: Iron-deficiency anemia (microcytes), pernicious anemia (macrocytes, B12 deficiency), aplastic anemia (bone marrow failure).
Excess destruction: Hemolytic anemias (thalassemias, sickle-cell anemia).
Polycythemia
Polycythemia is an abnormal excess of RBCs, increasing blood viscosity and causing sluggish flow. It may be caused by bone marrow cancer (polycythemia vera) or secondary to low oxygen levels or increased EPO.
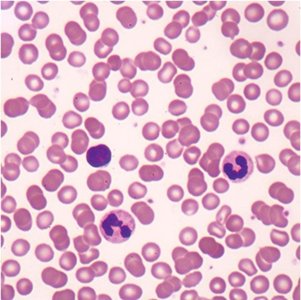
Leukocytes (White Blood Cells)
Structure and Function
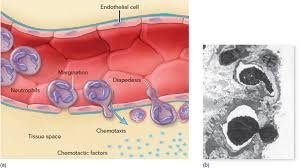
Leukocytes are complete cells with nuclei and organelles, making up less than 1% of blood volume. They defend against disease, can leave capillaries (diapedesis), and are attracted to infection sites (chemotaxis).
Leukocytosis: Elevated WBC count (>11,000/μl), normal response to infection.
Two categories: Granulocytes (neutrophils, eosinophils, basophils) and agranulocytes (lymphocytes, monocytes).
Granulocytes
Neutrophils: Most numerous, phagocytic, kill bacteria by respiratory burst.
Eosinophils: Digest parasitic worms, modulate immune response, involved in allergies/asthma.
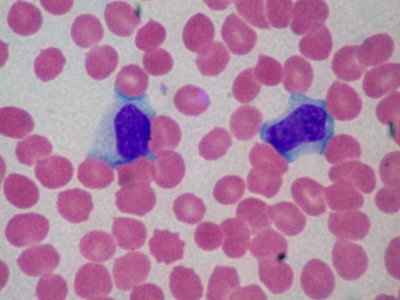
Basophils: Rarest, release histamine and heparin, trigger allergic responses.

Agranulocytes
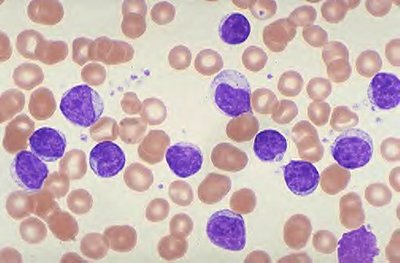
Lymphocytes: Crucial to immunity; T cells attack infected/tumor cells, B cells produce antibodies.
Monocytes: Largest WBCs, differentiate into macrophages, phagocytic, activate lymphocytes.
Leukocyte Production (Leukopoiesis)
Leukopoiesis is stimulated by interleukins and colony-stimulating factors (CSFs). All leukocytes originate from hemocytoblasts, branching into lymphoid (lymphocytes) and myeloid (other WBCs) lines.
Leukocyte Disorders
Leukemias: Cancers of bone marrow, overproduction of abnormal WBCs, classified as myeloid or lymphocytic, acute or chronic.
Infectious mononucleosis: Viral disease (Epstein-Barr virus), high numbers of enlarged lymphocytes, symptoms include fatigue, sore throat, low fever.
Leukopenia: Abnormally low WBC count, often drug-induced.


Platelets
Structure and Function
Platelets are fragments of megakaryocytes, essential for clotting. They form temporary plugs in vessel breaks and release chemicals to promote clotting and healing. Platelet formation is stimulated by thrombopoietin.
Normal count: 150,000–400,000 platelets/ml blood.
Lifespan: Degenerate in 10 days.
Hemostasis (Stopping Bleeding)
Steps of Hemostasis
Hemostasis is a rapid series of reactions to stop bleeding, involving four steps:
Vascular spasm: Vasoconstriction limits blood loss.
Platelet plug formation: Platelets adhere to collagen, aggregate, and release chemicals.
Coagulation: Reinforces plug with fibrin threads, transforming blood from liquid to gel.
Clot retraction and fibrinolysis: Clot is stabilized and removed after repair.

Coagulation Pathways
Coagulation involves intrinsic and extrinsic pathways, both leading to the formation of prothrombin activator, which converts prothrombin to thrombin. Thrombin then converts fibrinogen to fibrin, forming the clot.
Intrinsic pathway: Triggered by exposed collagen or activated platelets.
Extrinsic pathway: Triggered by tissue factor (TF) from damaged cells.
Common pathway: Factor Xa, Va, Ca2+, and platelet phospholipids form prothrombin activator.
Key Equations:
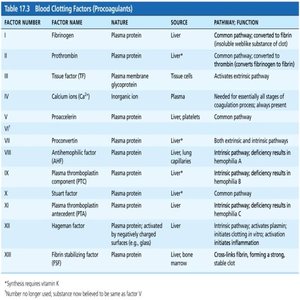
Blood Clotting Factors
Most clotting factors are plasma proteins produced by the liver and require vitamin K for synthesis. They are numbered I to XIII.
Factor Number | Factor Name | Source | Function |
|---|---|---|---|
I | Fibrinogen | Liver | Forms fibrin mesh |
II | Prothrombin | Liver | Converted to thrombin |
III | Tissue Factor (TF) | Tissue cells | Initiates extrinsic pathway |
IV | Calcium ions (Ca2+) | Plasma | Required for all stages |
V | Proaccelerin | Liver | Common pathway |
VIII | Antihemophilic factor | Liver | Intrinsic pathway |
IX | Plasma thromboplastin component | Liver | Intrinsic pathway |
X | Stuart factor | Liver | Common pathway |
XIII | Fibrin-stabilizing factor | Liver | Cross-links fibrin |
Clot Retraction and Fibrinolysis
Clot retraction occurs as platelets contract, pulling fibrin strands and squeezing serum from the clot. Platelet-derived growth factor (PDGF) and vascular endothelial growth factor (VEGF) stimulate vessel repair. Fibrinolysis removes clots after repair, with plasminogen converted to plasmin (fibrin-digesting enzyme).
Disorders of Hemostasis
Thromboembolic Disorders
Undesirable clot formation can lead to thrombus (clot in unbroken vessel) or embolus (floating clot). Risk factors include atherosclerosis, inflammation, and slow blood flow. Anticoagulant drugs (aspirin, heparin, warfarin) are used to prevent clotting.
Bleeding Disorders
Thrombocytopenia: Low platelet count, causes petechiae (small hemorrhages).
Impaired liver function: Inability to synthesize clotting factors, often due to vitamin K deficiency, hepatitis, or cirrhosis.
Hemophilia: Genetic disorder, deficiency of clotting factors (VIII, IX, XI), causes prolonged bleeding.
Disseminated intravascular coagulation (DIC): Both widespread clotting and severe bleeding.


Transfusing Red Blood Cells
Blood Groups and Typing
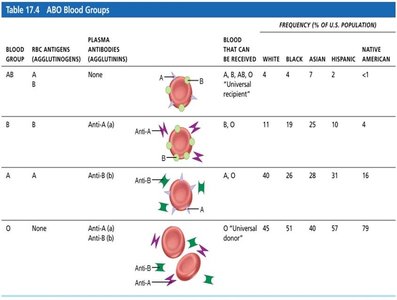
Human blood groups are determined by antigens (agglutinogens) on RBC membranes. The ABO and Rh groups are most important for transfusion compatibility.
ABO groups: Type A (A antigen), Type B (B antigen), Type AB (both), Type O (neither).
Antibodies: Present against antigens not found on individual's RBCs.
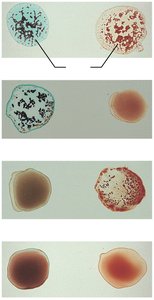
Transfusion reactions: Occur if mismatched blood is infused, leading to agglutination and hemolysis.
Blood Group | RBC Antigens | Plasma Antibodies | Blood That Can Be Received |
|---|---|---|---|
AB | A, B | None | A, B, AB, O |
B | B | Anti-A | B, O |
A | A | Anti-B | A, O |
O | None | Anti-A, Anti-B | O |
Rh Blood Groups
Rh+ indicates presence of D antigen. Anti-Rh antibodies form only after exposure to Rh+ blood. Hemolytic disease of the newborn (erythroblastosis fetalis) occurs when an Rh– mother carries an Rh+ fetus; RhoGAM serum prevents this reaction.
Case Studies
Anemia Case Study
A patient with chronic atrophic gastritis develops pernicious anemia due to lack of intrinsic factor, resulting in enlarged, non-dividing RBCs (macrocytes) and symptoms of fatigue, dizziness, and tachycardia.
Hemorrhage Case Study
A patient with severe bleeding receives saline transfusion, which dilutes blood and lowers hematocrit, requiring further observation and possible blood transfusion.
Additional info: This guide covers the structure, function, and disorders of blood as outlined in Chapter 17 of Human Anatomy & Physiology, including clinical applications and case studies relevant to college-level anatomy and physiology courses.
