 Back
BackBones and Bone Tissue: Structure, Function, and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Bones and Bone Tissue
Introduction to the Skeletal System
The skeletal system is a complex organ system that includes bones, joints, and supporting tissues. Bones are the main organs, with adults typically having 206 bones. Each bone is composed of bone (osseous) tissue, dense regular and irregular connective tissue, and bone marrow.
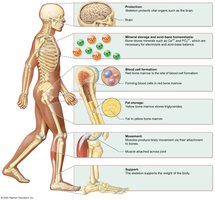
Functions of the Skeletal System
Protection: Bones such as the skull, sternum, and ribs protect vital organs.
Mineral Storage and Acid-Base Homeostasis: Bones store minerals (calcium, phosphorus, magnesium) essential for electrolyte and acid-base balance.
Blood Cell Formation: Red bone marrow is the site of hematopoiesis (blood cell production).
Fat Storage: Yellow bone marrow stores triglycerides in adipocytes.
Movement: Bones serve as attachment sites for muscles, enabling movement at joints.
Support: The skeleton provides structural support for the body.
Bone Structure
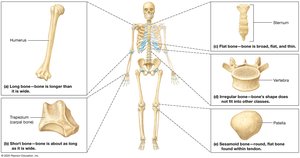
Classification by Shape
Long Bones: Longer than wide (e.g., humerus, femur).
Short Bones: About as long as wide (e.g., wrist, ankle bones).
Flat Bones: Thin and broad (e.g., skull, pelvis).
Irregular Bones: Complex shapes (e.g., vertebrae).
Sesamoid Bones: Small, oval-shaped, within tendons (e.g., patella).
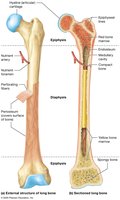
Structure of a Long Bone
Periosteum: Outer membrane of dense irregular connective tissue with blood vessels and nerves.
Perforating Fibers: Collagen anchors attaching periosteum to bone matrix.
Diaphysis: Shaft containing the medullary (marrow) cavity lined by endosteum and filled with marrow.
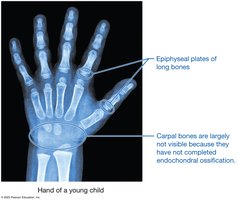
Epiphyses: Ends of the bone, filled with red marrow and covered with articular cartilage (hyaline cartilage).
Compact Bone: Dense outer layer resisting compression and twisting.
Spongy (Cancellous) Bone: Inner honeycomb-like structure housing bone marrow.
Epiphyseal Lines: Remnants of the growth plate (hyaline cartilage) in adults.
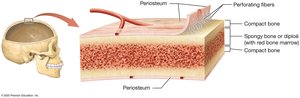
Structure of Short, Flat, Irregular, and Sesamoid Bones
These bones share similarities with long bones but have fewer structures. In flat bones, the spongy bone is called diploë. Some skull bones contain sinuses to reduce weight.
Blood and Nerve Supply to Bone
Supplied by blood vessels in the periosteum and nutrient arteries entering through the nutrient foramen.
Short, flat, irregular, and sesamoid bones receive blood mainly from periosteal vessels.
Red and Yellow Marrow
Red Marrow: Site of hematopoiesis; abundant in children, limited to certain bones in adults.
Yellow Marrow: Contains adipocytes and blood vessels; increases with age.
The Extracellular Matrix of Bone
Inorganic Matrix
Comprises ~65% of bone weight.
Mainly calcium and phosphorus in the form of hydroxyapatite crystals (), providing strength and resistance to compression.
Also contains bicarbonate, potassium, magnesium, and sodium salts.
Organic Matrix (Osteoid)
Comprises ~35% of bone weight.
Contains collagen fibers, proteoglycans, glycosaminoglycans, glycoproteins, and bone-specific proteins (e.g., osteocalcin).
Collagen resists torsion and tensile forces; osteocalcin organizes the inorganic matrix.

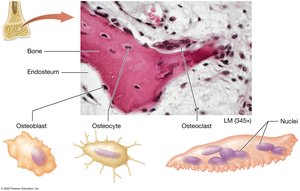
Bone Cells
Osteoblasts: Derived from osteogenic cells; build bone by secreting organic matrix and aiding inorganic matrix formation.
Osteocytes: Mature osteoblasts trapped in lacunae; maintain ECM and signal bone remodeling.
Osteoclasts: Large, multinucleated cells from bone marrow; break down bone ECM via bone resorption.


Osteopetrosis
Osteopetrosis ("marble bone disease") results from defective osteoclasts, leading to increased but brittle bone mass. Infantile forms can be fatal due to nerve entrapment and marrow failure; adult forms cause pain and fractures.

Histology of Bone
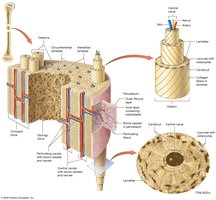
Compact Bone
Composed of osteons (Haversian systems) with concentric lamellae, central canals, lacunae, and canaliculi.
Interstitial and circumferential lamellae strengthen bone; perforating (Volkmann) canals connect osteons.
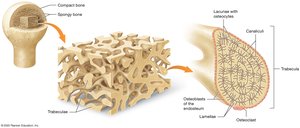
Spongy Bone
Consists of trabeculae with lamellae, lacunae, and canaliculi but lacks central canals.
Blood supply comes from bone marrow vessels.
Bone Formation: Ossification
Primary vs. Secondary Bone
Primary (Woven) Bone: Immature, irregular collagen, little inorganic matrix.
Secondary (Lamellar) Bone: Mature, organized lamellae, higher inorganic content.
Types of Ossification
Intramembranous Ossification: Forms flat bones (e.g., skull, clavicles) from mesenchymal membrane; spongy bone forms first.
Endochondral Ossification: Forms most bones below the head from a hyaline cartilage model; compact bone forms first.
Steps of Intramembranous Ossification
Osteoblasts develop in the primary ossification center from mesenchymal cells.
Osteoblasts secrete organic matrix, which calcifies; trapped osteoblasts become osteocytes.
Osteoblasts lay down trabeculae of early spongy bone; some mesenchyme becomes periosteum.
Osteoblasts in periosteum lay down early compact bone; matrix is remodeled.


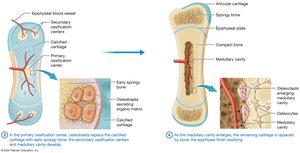
Steps of Endochondral Ossification
Chondroblasts in perichondrium differentiate into osteoblasts.
Osteoblasts build a bone collar; internal cartilage calcifies and chondrocytes die.
Osteoblasts replace calcified cartilage with early spongy bone; secondary ossification centers and medullary cavity develop.
Remaining cartilage is replaced by bone; epiphyses finish ossifying; cartilage remains at epiphyseal plates and articular surfaces.

Comparison Table: Intramembranous vs. Endochondral Ossification
Feature | Intramembranous | Endochondral |
|---|---|---|
Bone Types | Flat bones (skull, clavicle) | Long, short, irregular bones |
Model | Mesenchymal membrane | Hyaline cartilage |
Order of Bone Formation | Spongy bone first | Compact bone first |
Bone Growth
Longitudinal Growth (Length)
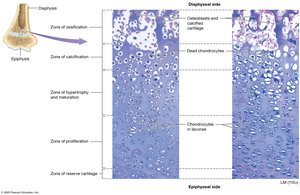
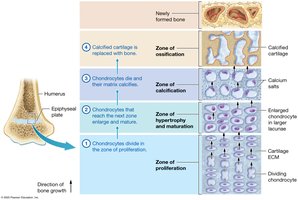
Occurs at the epiphyseal plate, which has five zones:
Zone of Reserve Cartilage
Zone of Proliferation (chondrocyte division)
Zone of Hypertrophy and Maturation (chondrocyte enlargement)
Zone of Calcification (chondrocyte death, matrix calcifies)
Zone of Ossification (osteoblasts build bone)
Appositional Growth (Width)
Osteoblasts in the periosteum lay down new circumferential lamellae, thickening the bone.
Osteoclasts enlarge the medullary cavity as bone thickens.
Hormonal Regulation of Bone Growth
Growth Hormone: Increases chondrocyte mitosis, osteogenic cell activity, and osteoblast activity.
Testosterone: Increases appositional growth and mitosis; accelerates epiphyseal plate closure.
Estrogen: Similar effects as testosterone but less pronounced; earlier epiphyseal plate closure.
Bone Remodeling
Overview
Bone remodeling is a continuous process involving bone deposition (by osteoblasts) and bone resorption (by osteoclasts). It maintains calcium homeostasis, repairs bone, replaces old bone, and adapts bone to stress.
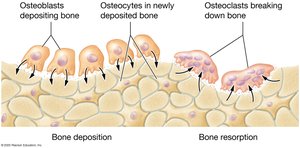
Bone Deposition
Osteoblasts secrete organic matrix and vesicles containing calcium, ATP, and enzymes, initiating calcification.
Bone Resorption
Osteoclasts secrete hydrogen ions (dissolve inorganic matrix) and enzymes (break down organic matrix).
Factors Influencing Bone Remodeling
Mechanical Stress: Compression and tension stimulate deposition; pressure stimulates resorption.
Hormones: Testosterone promotes deposition; estrogen inhibits osteoclasts.
Age: Hormone levels decline, reducing bone formation.
Nutrient Intake: Calcium, vitamin D, K, C, and protein are essential for healthy bone remodeling.

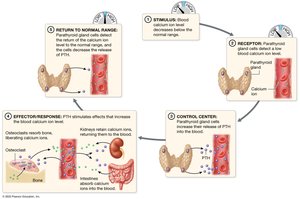
Calcium Homeostasis
Parathyroid Hormone (PTH): Increases blood calcium by stimulating bone resorption, increasing intestinal absorption, and reducing urinary loss.
Calcitonin: Decreases blood calcium by stimulating bone deposition (less potent in adults).
Bone Repair
Steps of Fracture Healing
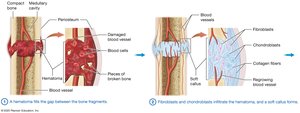
Hematoma formation: Blood fills the fracture gap, bone cells die.
Soft callus formation: Fibroblasts and chondroblasts produce connective tissue and cartilage.
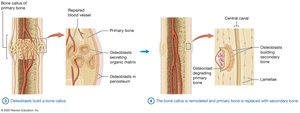
Bone callus formation: Osteoblasts lay down primary bone.
Remodeling: Primary bone is replaced by secondary bone.
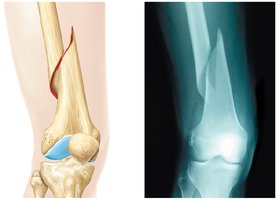
Types of Fractures
Type | Description |
|---|---|
Simple (Closed) | Skin and tissue remain intact |
Compound (Open) | Skin and tissue are damaged |
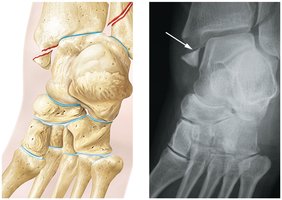
Transverse | Fracture is perpendicular to bone's long axis |
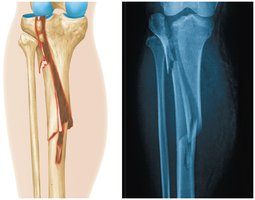
Spiral | Fracture spirals around the bone |
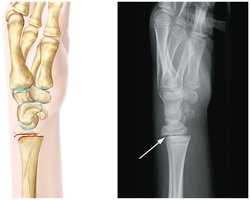
Comminuted | Bone is shattered into multiple pieces |
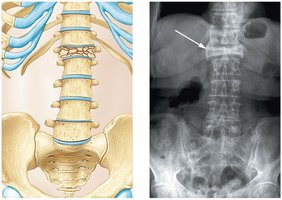
Compression | Bone is crushed (often in vertebrae) |
Greenstick | Bone breaks on one side, bends on the other (common in children) |
Epiphyseal Plate | Fracture involves the growth plate |

Treatment of Fractures
Closed Reduction: Bone ends are aligned without surgery.
Open Reduction: Surgical fixation with plates, wires, or screws.
Clinical Correlations
Osteoporosis: Inadequate inorganic matrix leads to brittle bones and increased fracture risk. Prevention includes adequate calcium/vitamin D, exercise, and medications.
Achondroplasia: Most common cause of dwarfism due to abnormal cartilage growth; results in short limbs and characteristic features.
Gigantism and Acromegaly: Excess growth hormone before (gigantism) or after (acromegaly) epiphyseal plate closure causes abnormal bone growth.
