 Back
BackBones and Skeletal Tissues: Structure, Function, Development, and Disorders
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Bones and Skeletal Tissues
Structure and Function of Bones
Bones are rigid organs that form the skeleton, providing support, protection, movement, mineral storage, and blood cell formation. Their structure is adapted to fulfill these functions efficiently.
Support: Bones provide a framework for the body and anchor muscles.
Protection: Bones protect vital organs (e.g., skull protects brain, ribs protect heart and lungs).
Movement: Bones act as levers for muscles to produce movement.
Mineral Storage: Bones store calcium and phosphorus, releasing them as needed.
Blood Cell Formation: Hematopoiesis occurs in red marrow cavities of certain bones.
Microscopic Anatomy of Bone: Bone Cells
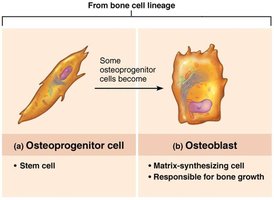
Bone tissue contains five major cell types, each with specialized functions in bone growth, maintenance, and remodeling.
Osteogenic (Osteoprogenitor) Cells: Stem cells found in periosteum and endosteum; differentiate into osteoblasts or bone-lining cells.
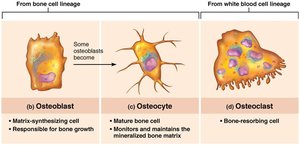
Osteoblasts: Bone-forming cells that secrete osteoid (unmineralized bone matrix composed mainly of collagen and calcium-binding proteins).
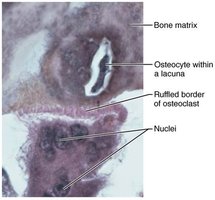
Osteocytes: Mature bone cells residing in lacunae; maintain bone matrix and act as stress sensors.
Bone-lining Cells: Flat cells on bone surfaces; help maintain bone matrix.
Osteoclasts: Multinucleate cells derived from hematopoietic stem cells; responsible for bone resorption.
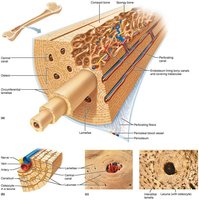
Microscopic Anatomy of Compact Bone
Compact bone is organized into structural units called osteons, which provide strength and support. It contains concentric lamellae, central canals, and canaliculi for nutrient and waste exchange.
Osteon (Haversian System): Fundamental unit of compact bone.
Lamellae: Layers of bone matrix.
Central Canal: Contains blood vessels and nerves.
Canaliculi: Tiny channels connecting osteocytes for communication.
Chemical Composition of Bone
Organic and Inorganic Components
Bones are composed of both organic and inorganic materials, each contributing to bone properties.
Organic Components: Include cells (osteogenic, osteoblasts, osteocytes, bone-lining cells, osteoclasts) and osteoid (collagen fibers and ground substance). Provide tensile strength and flexibility.
Inorganic Components: Mainly hydroxyapatites (calcium phosphate crystals). Provide hardness and resistance to compression.
Example: Bone is half as strong as steel in resisting compression and as strong as steel in resisting tension.
Bone Development (Ossification)
Formation of the Bony Skeleton
Bone tissue formation (ossification) begins in the embryo and continues throughout life. Two main processes are involved: endochondral and intramembranous ossification.
Endochondral Ossification: Bone forms by replacing hyaline cartilage; forms most bones below the skull except clavicles.
Intramembranous Ossification: Bone develops from fibrous membranes; forms flat bones of the skull and clavicle.
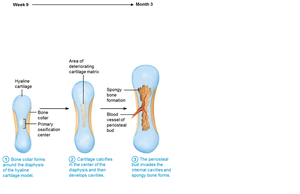
Endochondral Ossification Steps
Bone collar forms around diaphysis of cartilage model.
Central cartilage in diaphysis calcifies and develops cavities.
Periosteal bud invades cavities, forming spongy bone.
Diaphysis elongates, medullary cavity forms, secondary ossification centers appear in epiphyses.
Epiphyses ossify; hyaline cartilage remains in epiphyseal plates and articular cartilages.



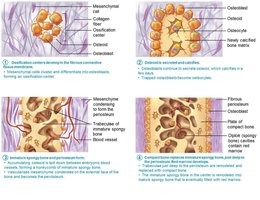
Intramembranous Ossification Steps
Ossification centers form as mesenchymal cells cluster and become osteoblasts.
Osteoid is secreted and calcified.
Woven bone forms around blood vessels, resulting in trabeculae.
Outer layer forms periosteum; lamellar bone replaces woven bone, red marrow appears.

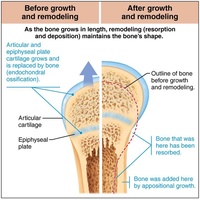
Postnatal Bone Growth
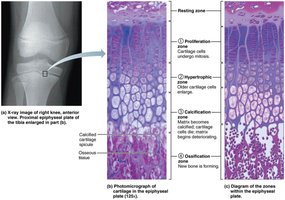
Growth in Length of Long Bones
Long bones grow in length by interstitial growth at the epiphyseal plate, which consists of five zones:
Resting (quiescent) zone
Proliferation (growth) zone
Hypertrophic zone
Calcification zone
Ossification (osteogenic) zone
Epiphyseal Plate Closure
Bone lengthening ceases when the epiphysis and diaphysis fuse, closing the epiphyseal plate. This occurs around age 18 in females and 21 in males.

Growth in Width (Appositional Growth)
Bones increase in thickness throughout life by appositional growth. Osteoblasts add bone matrix to the external surface, while osteoclasts remove bone from the internal surface.
Hormonal Regulation of Bone Growth
Growth Hormone: Stimulates epiphyseal plate activity.
Thyroid Hormone: Modulates growth hormone activity.
Sex Hormones: Promote growth spurts and induce epiphyseal plate closure.
Bone Remodeling
Bone Deposit and Resorption
Bone remodeling is a continuous process involving bone deposit by osteoblasts and bone resorption by osteoclasts. About 5–7% of bone mass is recycled weekly.
Bone Deposit: New matrix deposited by osteoblasts; triggered by mechanical signals, calcium/phosphate concentrations, matrix proteins, and alkaline phosphatase.
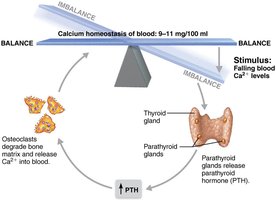
Bone Resorption: Osteoclasts break down matrix, secrete enzymes and acids, and release calcium into blood.
Control of Remodeling
Hormonal Controls
Parathyroid Hormone (PTH): Released in response to low blood calcium; stimulates osteoclasts to resorb bone.
Calcitonin: Released in response to high blood calcium; effects are minor except at high doses.
Leptin and Serotonin: Influence bone density and turnover.
Response to Mechanical Stress
Bone adapts to mechanical stress according to Wolf’s law: bones grow or remodel in response to demands placed on them. Stress causes electrical signals and fluid flow changes that stimulate remodeling.
Example: Weight lifters develop thicker bones at muscle attachment sites; bones of bedridden individuals are featureless due to lack of stress.

Bone Disorders
Osteomalacia and Rickets
Osteomalacia (in adults) and rickets (in children) are conditions where bones are poorly mineralized, resulting in soft, weak bones. Rickets causes bone deformities due to vitamin D deficiency or insufficient calcium.
Osteoporosis
Osteoporosis is characterized by bone resorption exceeding bone deposit, leading to decreased bone mass and increased fracture risk. Most common in aged, postmenopausal women.
Risk Factors: Age, gender, low exercise, poor diet, smoking, genetics, hormone-related conditions.
Treatments: Calcium, vitamin D, exercise, hormone therapy, bisphosphonates, denosumab.
Prevention: Adequate calcium intake, reduced alcohol, weight-bearing exercise.

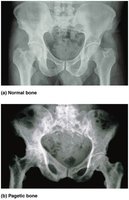
Paget’s Disease
Paget’s disease involves excessive and disorganized bone remodeling, resulting in weak, deformed bones. Most commonly affects spine, pelvis, femur, and skull. Treatment includes calcitonin and bisphosphonates.
Developmental and Age-Related Aspects of Bone
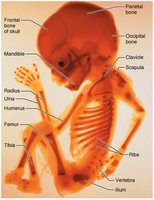
Embryonic and Fetal Development
Embryonic skeleton ossifies predictably, allowing fetal age determination by imaging. Most long bones begin ossifying by 8 weeks, with primary ossification centers developed by week 12.
Birth to Adulthood
At birth, most long bones are ossified except at epiphyses.
Epiphyseal plates persist through childhood and adolescence.
By age 25, all bones are completely ossified and skeletal growth ceases.
Age-Related Changes
Bone formation exceeds resorption in children and adolescents.
Bone mass, mineralization, and healing ability decrease with age, especially after the fourth decade.
Bone loss is greater in females and individuals of white ethnicity.
Bone Cell Type | Function | Origin |
|---|---|---|
Osteogenic Cell | Stem cell; differentiates into osteoblasts | Bone cell lineage |
Osteoblast | Matrix-synthesizing cell; responsible for bone growth | Bone cell lineage |
Osteocyte | Mature bone cell; maintains bone matrix | Bone cell lineage |
Osteoclast | Bone-resorbing cell | White blood cell lineage |
Disorder | Cause | Symptoms | Treatment |
|---|---|---|---|
Osteomalacia/Rickets | Vitamin D deficiency, insufficient calcium | Soft, weak bones; bone deformities | Vitamin D and calcium supplementation |
Osteoporosis | Bone resorption exceeds deposit | Decreased bone mass, fractures | Calcium, vitamin D, exercise, medications |
Paget's Disease | Unknown, possibly viral | Weak, deformed bones | Calcitonin, bisphosphonates |
Key Equations
Calcium Homeostasis:
Bone Remodeling:
Additional info: Tables and equations were expanded for clarity and completeness. All images included are directly relevant to the adjacent content and reinforce key concepts in bone structure, development, and disorders.
