 Back
BackCardiac Output, Stroke Volume, and Cardiac Physiology: ANP Study Guide
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Module 4, Part 3
Cardiac Output and Stroke Volume
Definitions and Basic Concepts
Cardiac output and stroke volume are fundamental concepts in cardiac physiology, describing the amount of blood pumped by the heart and the factors influencing this process.
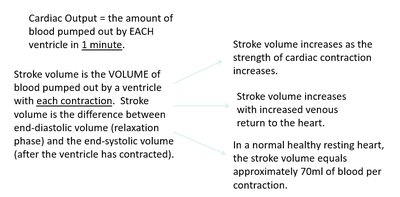
Cardiac Output (CO): The amount of blood pumped out by each ventricle in one minute.
Stroke Volume (SV): The volume of blood pumped out by a ventricle with each contraction. It is calculated as the difference between end-diastolic volume (EDV) and end-systolic volume (ESV).
EDV: The amount of blood collected in a ventricle during diastole (relaxation phase), typically about 120 mL.
ESV: The amount of blood remaining in a ventricle after contraction (systole), typically about 50 mL.
SV Calculation:
Normal SV: In a healthy, resting heart, stroke volume is approximately 70 mL per contraction.
Key Points:
Stroke volume increases as the strength of cardiac contraction increases.
Stroke volume increases with increased venous return to the heart.
Cardiac output is the product of heart rate and stroke volume:
Regulation of Stroke Volume
Intrinsic Control
Intrinsic control refers to the heart's inherent ability to vary stroke volume based on the degree of stretch of cardiac muscle fibers.
Length-Tension Relationship: Stretching cardiac muscle fibers increases the number of active crossbridge attachments, enhancing contraction strength.
Venous Return: The amount of blood returning to the heart stretches the ventricles, affecting stroke volume.
Frank-Starling Law: The more the heart muscle is stretched (within physiological limits), the greater the force of contraction.
Example: A slow heart rate allows more time for ventricular filling, increasing EDV and stroke volume. Exercise increases venous return, also boosting stroke volume.
Extrinsic Control
Extrinsic control involves regulation by the autonomic nervous system, particularly sympathetic stimulation.
Sympathetic Stimulation: Increases heart rate and force of contraction via norepinephrine and epinephrine release.
Parasympathetic Stimulation: Reduces heart rate and contractility via acetylcholine release from the vagus nerve.
Vagal Tone: Under resting conditions, the heart exhibits vagal tone, resulting in a slower heart rate.
Preload, Contractility, and Afterload
Preload
Preload is the stretching of ventricular muscle fibers due to blood volume at end-diastole. It is a key determinant of contractility and stroke volume.
Preload: The extent to which the heart is stretched as it fills during diastole.
Influence: Preload is dependent on heart rate and venous return.
Contractility: The ability of the myocardium to contract normally, influenced by preload.
Example: More air in a balloon results in a more forceful release, analogous to increased preload leading to stronger heart contractions.
Afterload
Afterload is the pressure the ventricles must overcome to eject blood into the aorta and pulmonary artery.
Afterload: The pressure required to open the semilunar valves and push blood out of the heart.
High Blood Pressure: Increases afterload, making it harder for the heart to pump blood, and decreases stroke volume.


Frank-Starling Law of the Heart
Intrinsic Relationship
The Frank-Starling Law describes the relationship between end-diastolic volume and stroke volume, ensuring equal outputs of the ventricles and proper blood distribution.
Law: The heart pumps all the blood returned to it; increased venous return increases stroke volume.
Mechanism: Increased stretch leads to increased force of contraction.
Cardiac Output
Calculation and Clinical Relevance
Cardiac output is a measure of the heart's efficiency and is crucial for maintaining adequate blood flow to tissues.
Formula:
Normal Values: Heart rate (HR) ≈ 75 beats/min, SV ≈ 70 mL/beat, so mL/min.
Cardiac Reserve: The ability of the heart to increase cardiac output above normal levels, typically 4x in non-athletes and up to 7x in athletes.
Transmyocardial Revascularization (TMR)
Innovative Surgical Approach
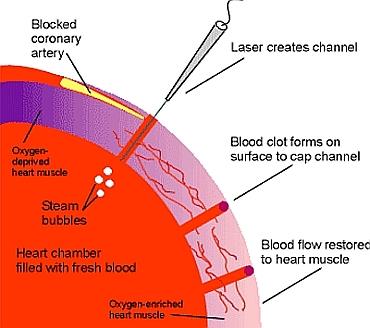
Transmyocardial revascularization (TMR) is a surgical procedure used to treat severe angina in patients who are not candidates for conventional heart surgery.
Procedure: A laser drills microscopic channels into the heart muscle, allowing blood flow to areas with poor circulation.
Effect: Blood clots form at the channel surface, preventing blood loss, and new blood flow supplies oxygen to the heart muscle.
Clinical Outcome: Most patients report significant improvement in symptoms post-surgery.

Summary Table: Factors Affecting Stroke Volume and Cardiac Output
Factor | Effect on Stroke Volume | Effect on Cardiac Output |
|---|---|---|
Increased Preload | Increases | Increases |
Increased Afterload | Decreases | Decreases |
Increased Contractility | Increases | Increases |
Decreased Venous Return | Decreases | Decreases |
Increased Heart Rate (short-term) | Increases | Increases |
Prolonged Tachycardia | Decreases | Decreases |
Additional info: Academic context was added to clarify the physiological mechanisms and clinical relevance of stroke volume, cardiac output, preload, afterload, and TMR. Examples and analogies (balloon, steam, reptiles) were expanded for student understanding.
