 Back
BackChapter 17: Blood – Structure, Function, and Clinical Aspects
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Blood: Internal Transport System
Overview and Functions
Blood is a specialized connective tissue that serves as the primary transport medium of the cardiovascular system. It is essential for maintaining homeostasis through its roles in transport, regulation, and protection.
Transport: Delivers oxygen and nutrients to cells, removes metabolic wastes, and transports hormones.
Regulation: Maintains body temperature, pH balance, and fluid volume.
Protection: Prevents blood loss via clotting and combats infection through immune cells and proteins.
Composition of Blood
Blood Components
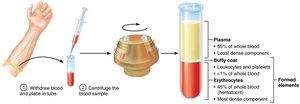
Blood consists of a liquid matrix called plasma and formed elements (cells and cell fragments). When centrifuged, blood separates into three layers:
Plasma: ~55% of blood volume; contains water, proteins, nutrients, hormones, and waste products.
Buffy coat: <1% of blood; contains leukocytes (white blood cells) and platelets.
Erythrocytes: ~45% of blood (hematocrit); red blood cells responsible for oxygen transport.
Physical Characteristics and Volume
Sticky, opaque fluid with a metallic taste.
Color varies with oxygen content: scarlet red (high O2), dark red (low O2).
pH: 7.35–7.45; constitutes ~8% of body weight.
Average volume: Males 5–6 L, Females 4–5 L.
Blood Plasma
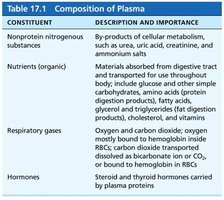
Plasma is a straw-colored, sticky fluid making up about 90% water and containing over 100 dissolved solutes. Plasma proteins, mainly produced by the liver, are the most abundant solutes and include:
Albumin (60%): Maintains osmotic pressure, acts as a carrier, and buffers blood pH.
Globulins (36%): Transport proteins and antibodies.
Fibrinogen (4%): Forms fibrin threads of blood clots.

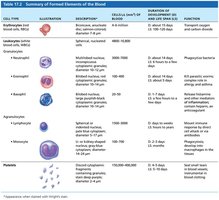
Formed Elements of Blood
Types and Characteristics
The formed elements include erythrocytes (RBCs), leukocytes (WBCs), and platelets. Only WBCs are complete cells; RBCs lack nuclei and organelles, and platelets are cell fragments. Most formed elements are short-lived and originate in the bone marrow.

Erythrocytes (Red Blood Cells)
Structure and Function
Erythrocytes are small, biconcave, anucleate cells specialized for gas transport. Their shape increases surface area for gas exchange, and they are filled with hemoglobin (Hb), which binds oxygen.
Biconcave shape: Maximizes surface area-to-volume ratio.
No mitochondria: ATP production is anaerobic, so RBCs do not consume the oxygen they carry.

Hemoglobin Structure and Oxygen Transport
Hemoglobin is a protein composed of four polypeptide chains (two alpha, two beta), each with a heme group containing an iron atom that binds oxygen. Each Hb molecule can carry four O2 molecules, and each RBC contains about 250 million Hb molecules.
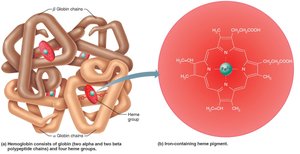
O2 loading in lungs: Forms oxyhemoglobin (bright red).
O2 unloading in tissues: Forms deoxyhemoglobin (dark red).
CO2 transport: 20% of CO2 binds to Hb, forming carbaminohemoglobin.
Erythropoiesis: Production of Erythrocytes
Erythropoiesis is the process of RBC formation, occurring in red bone marrow. It involves several stages from hematopoietic stem cells to mature erythrocytes:
Hematopoietic stem cell → Myeloid stem cell → Proerythroblast → Basophilic erythroblast → Polychromatic erythroblast → Orthochromatic erythroblast → Reticulocyte → Erythrocyte

Regulation of Erythropoiesis
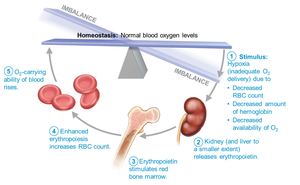
RBC production is regulated by erythropoietin (EPO), a hormone produced mainly by the kidneys in response to hypoxia (low oxygen levels). EPO stimulates the bone marrow to increase RBC production. Adequate supplies of iron, vitamin B12, and folic acid are required for effective erythropoiesis.
Life Cycle and Fate of Erythrocytes
RBCs have a lifespan of 100–120 days. Old RBCs are removed by macrophages in the spleen, and their components are recycled: iron is stored, heme is converted to bilirubin (excreted in bile), and globin is broken down into amino acids.

Erythrocyte Disorders
Anemia: Reduced oxygen-carrying capacity due to blood loss, decreased production, or increased destruction of RBCs. Types include iron-deficiency, pernicious, renal, aplastic, hemolytic, thalassemias, and sickle-cell anemia.
Polycythemia: Excess RBCs increase blood viscosity, leading to sluggish blood flow. Causes include bone marrow cancer, high altitude, or blood doping.

Leukocytes (White Blood Cells)
Structure and Function
Leukocytes are complete cells that defend the body against infection. They can leave the bloodstream (diapedesis) and move toward infection sites (chemotaxis). There are two main categories: granulocytes and agranulocytes.
Granulocytes
Neutrophils: Most abundant; phagocytize bacteria.
Eosinophils: Combat parasitic worms; involved in allergies and asthma.
Basophils: Release histamine; involved in inflammatory responses.

Agranulocytes
Lymphocytes: T cells (attack infected/tumor cells), B cells (produce antibodies).
Monocytes: Differentiate into macrophages; phagocytize pathogens and debris.

Leukopoiesis: Production of Leukocytes
Leukopoiesis is stimulated by interleukins and colony-stimulating factors (CSFs). All leukocytes originate from hemocytoblasts and differentiate into myeloid or lymphoid lineages.

Leukocyte Disorders
Leukopenia: Abnormally low WBC count, often drug-induced.
Leukemias: Cancers of WBCs; classified as myeloid or lymphocytic, acute or chronic.
Infectious mononucleosis: Viral disease causing high numbers of atypical lymphocytes.
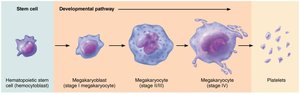
Platelets
Structure and Function
Platelets are fragments of megakaryocytes and are essential for blood clotting. They form temporary plugs to seal vessel breaks and release chemicals that promote clotting.
Normal count: 150,000–400,000/μL blood.
Regulated by thrombopoietin.
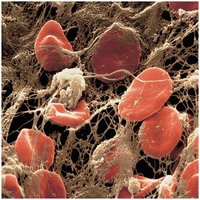
Hemostasis: Stoppage of Bleeding
Three Major Steps
Vascular spasm: Vasoconstriction reduces blood flow after vessel injury.
Platelet plug formation: Platelets adhere to exposed collagen, become activated, and aggregate.
Coagulation: Fibrin threads reinforce the platelet plug, forming a stable clot.

Coagulation Pathways
Coagulation involves a cascade of clotting factors, leading to the conversion of fibrinogen to fibrin. There are intrinsic and extrinsic pathways, both converging on the activation of factor X to form prothrombin activator.


Clot Retraction and Fibrinolysis
Clot retraction: Platelets contract, pulling wound edges together and squeezing out serum.
Fibrinolysis: Plasmin digests fibrin, dissolving the clot after repair is complete.
Factors Limiting Clot Growth and Formation
Swift removal and dilution of clotting factors.
Inhibition of activated clotting factors by antithrombin III and heparin.
Prevention of platelet adhesion by smooth endothelium and antithrombic substances.
Disorders of Hemostasis
Thromboembolic Disorders
Thrombus: Clot in an unbroken vessel; may block circulation.
Embolus: Freely floating clot; can cause embolism if it lodges in a vessel.
Anticoagulant drugs: Aspirin, heparin, and warfarin are used to prevent clot formation.
Bleeding Disorders
Thrombocytopenia: Low platelet count, leading to petechiae (small hemorrhages).
Impaired liver function: Reduces synthesis of clotting factors.
Hemophilia: Hereditary bleeding disorders due to deficiencies in clotting factors VIII, IX, or XI.
Disseminated intravascular coagulation (DIC): Involves both widespread clotting and bleeding.

Blood Transfusions and Blood Groups
ABO and Rh Blood Groups
Blood groups are determined by the presence or absence of antigens (agglutinogens) on RBC membranes. The ABO system is based on A and B antigens, while the Rh system is based on the D antigen.
Type A: A antigen, anti-B antibody
Type B: B antigen, anti-A antibody
Type AB: Both antigens, no antibodies (universal recipient)
Type O: No antigens, both antibodies (universal donor)
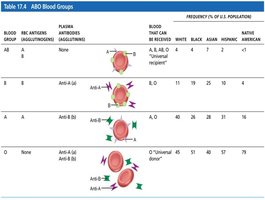
Blood Typing and Transfusion Reactions
Blood typing involves mixing blood with anti-A and anti-B sera to detect agglutination. Transfusion reactions occur if mismatched blood is given, leading to agglutination and hemolysis of donor RBCs.

Diagnostic Blood Tests
Hematocrit: Measures RBC percentage; low in anemia.
Blood glucose: Assesses diabetes.
Differential WBC count: Identifies proportions of WBC types.
Prothrombin time and platelet count: Assess hemostasis.
Comprehensive medical panel (CMP): Checks blood chemistry for organ function.
Complete blood count (CBC): Evaluates overall blood health.
Developmental Aspects of Blood
Fetal blood cells are initially formed in the yolk sac, liver, and spleen, with red bone marrow becoming the primary site by the seventh month. Fetal hemoglobin (HbF) has a higher affinity for oxygen than adult hemoglobin (HbA). Blood diseases in aging include chronic leukemias, anemias, and clotting disorders, often secondary to other systemic diseases.
