 Back
BackChapter 17: The Heart – Structure, Function, and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Cardiovascular System: The Heart
Overview and Functions
The heart is a muscular organ responsible for pumping blood throughout the body, maintaining circulation, and ensuring the delivery of oxygen and nutrients. It beats approximately 100,000 times per day, moving about 8,000 liters of blood.
Generating Blood Pressure: Essential for blood flow through vessels.
Routing Blood: Separates pulmonary (lungs) and systemic (body) circulations.
Ensuring One-Way Flow: Heart valves prevent backflow.
Regulating Blood Supply: Adjusts output based on body needs.
Pulmonary and Systemic Circuits
The heart operates two main circuits:
Pulmonary Circuit: Right side pumps deoxygenated blood to lungs for gas exchange.
Systemic Circuit: Left side pumps oxygenated blood to the body.
Key Steps:
Deoxygenated blood is pumped to the lungs by the right heart.
Gas exchange occurs in pulmonary capillaries.
Oxygenated blood returns to the left heart and is pumped to the body.
Gas exchange occurs in systemic capillaries; deoxygenated blood returns to the right heart.
Heart Anatomy and Structure
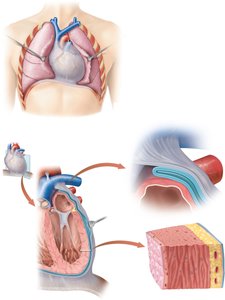
Pericardium and Heart Wall Layers
The heart is enclosed in the pericardium, a protective sac with two main layers:
Fibrous Pericardium: Tough, outer layer; prevents overdistention and anchors the heart.
Serous Pericardium: Thin, inner layer; divided into parietal (lines fibrous layer) and visceral (covers heart surface, also called epicardium).
Pericardial Cavity: Space between layers, filled with pericardial fluid to reduce friction.
Three Layers of the Heart Wall:
Epicardium: Smooth outer surface (visceral pericardium).
Myocardium: Middle layer, composed of cardiac muscle cells; responsible for contraction.
Endocardium: Smooth inner surface lining heart chambers.
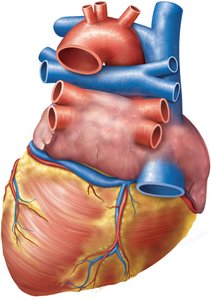
External Anatomy of the Heart
The heart has distinct external features, including major vessels and coronary arteries.
Major Vessels: Superior/inferior vena cava, pulmonary trunk, pulmonary veins, aorta.
Auricles: Extensions of atria.
Coronary Arteries: Supply blood to heart muscle.
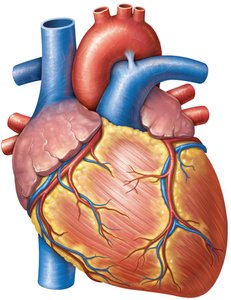
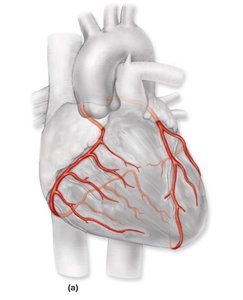
Coronary Circulation
The heart receives its own blood supply via the coronary arteries and veins.
Left Coronary Artery: Branches into circumflex and anterior interventricular arteries.
Right Coronary Artery: Branches into marginal and posterior interventricular arteries.
Coronary Sinus: Collects venous blood from the heart muscle.
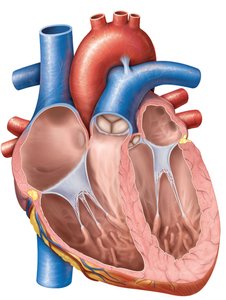
Internal Anatomy: Chambers, Valves, and Muscles
The heart has four chambers (right/left atria and ventricles) and four main valves:
Aortic Semilunar Valve
Pulmonary Semilunar Valve
Bicuspid (Mitral) Valve
Tricuspid Valve
Muscles include pectinate, trabeculae carneae, and papillary muscles.
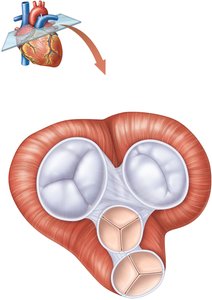
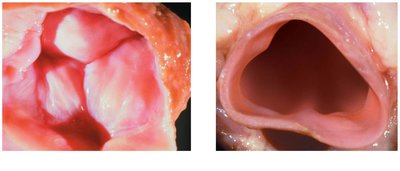
Heart Valves and Fibrous Skeleton
Valves ensure one-way blood flow and are supported by a fibrous skeleton:
Atrioventricular Valves: Tricuspid and mitral (bicuspid) valves, located between atria and ventricles.
Semilunar Valves: Aortic and pulmonary valves, located at the bases of large arteries.
Fibrous Skeleton: Plate of connective tissue providing support, electrical insulation, and muscle attachment.
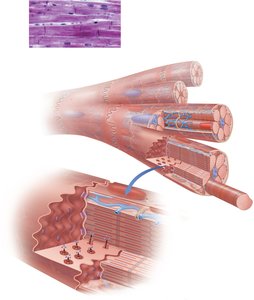
Cardiac Muscle Histology
Structure and Function
Cardiac muscle cells are specialized for contraction and electrical conduction:
Intercalated Discs: Specialized cell-cell contacts; membranes interdigitate.
Desmosomes: Hold cells together.
Gap Junctions: Allow action potentials to move between cells.
Two types of cardiac muscle cells:
Contractile Cells: Propel blood.
Auto-rhythmic Cells: Control and coordinate heartbeat.
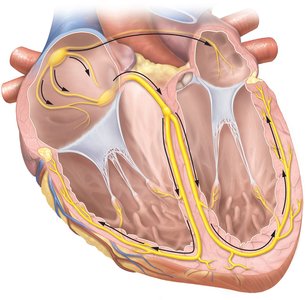
Cardiac Conducting System
Electrical Pathways
The heart's conducting system coordinates contraction:
Sinoatrial (SA) Node: Generates action potentials, spreads to atrial cells and AV node.
Atrioventricular (AV) Node: Delays impulse, then sends to AV bundle and bundle branches.
Purkinje Fibers: Spread impulse to ventricular contractile cells.
Cardiac Cycle
The cardiac cycle is the repetitive process of contraction and relaxation:
Systole: Contraction phase.
Diastole: Relaxation phase.
Cardiac Action Potentials and Muscle Contraction
Phases of Cardiac Action Potential
Cardiac muscle action potentials have distinct phases:
Depolarization: Voltage-gated Na+ channels open.
Plateau: Voltage-gated Ca2+ channels open, prolonging depolarization.
Repolarization: Voltage-gated K+ channels open, restoring resting potential.

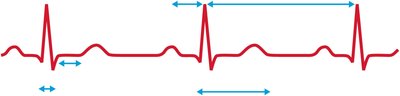
Electrocardiogram (ECG)
An ECG records electrical events in the heart:
P Wave: Atrial depolarization.
QRS Complex: Ventricular depolarization.
T Wave: Ventricular repolarization.
PR Interval: Atria contract and relax, ventricles begin contraction.
QT Interval: Ventricles contract and relax.
RR Interval: Duration of a cardiac action potential.
Cardiac Cycle and Heart Sounds
Phases of the Cardiac Cycle
Ventricular Filling: Atria contract, ventricles fill.
Isovolumetric Contraction: Ventricles contract, AV valves close.
Ventricular Ejection: Semilunar valves open, blood ejected.
Isovolumetric Relaxation: Ventricles relax, semilunar valves close.
Heart Sounds
S1 (Lubb): AV valves close at start of ventricular systole.
S2 (Dupp): Semilunar valves close at start of ventricular diastole.
S3: Occasional, due to turbulent blood flow.
Murmurs: Due to valve regurgitation (backflow).
Cardiac Output and Regulation
Cardiac Output Formula
Cardiac output (CO) is the volume of blood pumped by the left ventricle per minute:
Formula:
HR: Heart rate (beats/min)
SV: Stroke volume (mL/beat)
Stroke Volume and Regulation
End-Diastolic Volume (EDV): Maximum blood in ventricles before contraction.
End-Systolic Volume (ESV): Blood remaining after contraction.
Mean Arterial Pressure (MAP):
Peripheral Resistance (PR): Resistance against which blood is pumped.
Intrinsic Regulation:
Preload: Stretch of ventricular walls; greater stretch increases force (Starling's law).
Afterload: Pressure ventricles must overcome to eject blood.
Extrinsic Regulation:
Parasympathetic Stimulation: Decreases heart rate via vagus nerve.
Sympathetic Stimulation: Increases heart rate and force via cardiac nerves.
Hormonal Control: Epinephrine and norepinephrine increase heart rate and force.
Heart Diseases and Disorders
Common Conditions
Pericarditis: Inflammation of pericardium, causes friction and pain.
Coronary Artery Disease (CAD): Blockage of coronary circulation.
Myocardial Infarction: Heart attack, usually from severe CAD.
Angina Pectoris: Chest pain due to reduced blood flow.
Congestive Heart Failure: Failure of ventricles to eject blood effectively.
Cardiac Edema: Blood backs up into lungs, causing shortness of breath.
Arrhythmias: Ectopic pacemaker, bradycardia, tachycardia.
Atheromas: Plaque build-up in arteries, can lead to arteriosclerosis.
Chronotropic Chemicals
Negative Chronotropic Agents: Decrease heart rate (e.g., parasympathetic activity, beta-blockers).
Positive Chronotropic Agents: Increase heart rate (e.g., sympathetic stimulation, thyroid hormone, caffeine, nicotine, cocaine).
Potassium (K+): Hyperkalemia slows heart rate; hypokalemia increases stimulation needed.
Calcium (Ca2+): Hypercalcemia decreases heart rate, increases contraction; hypocalcemia increases heart rate, decreases contraction.
Summary Table: Heart Valves and Sounds
Valve | Location | Sound Timing |
|---|---|---|
Aortic | 2nd intercostal space, right sternal border | S2 |
Tricuspid | 5th intercostal space, left sternal border | S1 |
Mitral | 5th intercostal space, mid-clavicular line | S1 |
Pulmonary | 2nd intercostal space, left sternal border | S2 |
Key Equations
Additional info:
Cardiac output is influenced by both intrinsic (preload, afterload) and extrinsic (neural, hormonal) factors.
Heart diseases often involve structural or functional abnormalities in the heart or its vessels.
