 Back
BackChapter 19: Blood – Structure, Function, and Clinical Relevance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Blood: Overview and Composition
Definition and General Properties
Blood is a fluid connective tissue that circulates continuously through the heart and blood vessels, comprising about 8% of total body weight and averaging 5 liters in volume in adults. It consists of a liquid extracellular matrix called plasma and formed elements (erythrocytes, leukocytes, and platelets).
Plasma: Pale yellow liquid, 90% water, contains proteins, nutrients, hormones, ions, and wastes.
Formed Elements: Erythrocytes (red blood cells), leukocytes (white blood cells), and platelets (cell fragments).
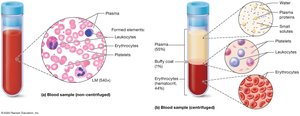
Blood Separation and Hematocrit
When centrifuged, blood separates into three layers:
Plasma: ~55% of blood volume (top layer)
Buffy Coat: ~1% (middle layer; leukocytes and platelets)
Erythrocytes: ~44% (bottom layer)
Hematocrit is the percentage of blood composed of erythrocytes, a key clinical measure.
Functions of Blood
Major Functions
Gas Exchange: Transports oxygen (O2) from lungs to tissues and carbon dioxide (CO2) from tissues to lungs.
Solute Distribution: Carries nutrients, hormones, ions, and wastes throughout the body.
Immune Function: Leukocytes and plasma proteins defend against pathogens.
Temperature Regulation: Distributes heat generated by metabolism.
Hemostasis: Platelets and proteins form clots to seal damaged vessels.
Acid-Base Homeostasis: Maintains blood pH (7.35–7.45) via buffer systems.
Blood Pressure Stabilization: Blood volume is a primary determinant of blood pressure.
Plasma and Plasma Proteins
Composition of Plasma
Plasma is 90% water, which determines blood viscosity. About 1% is small solutes (glucose, amino acids, ions, gases), and 9% is plasma proteins (mainly produced by the liver).
Albumin: Maintains colloid osmotic pressure, drawing water into blood.
Immune Proteins (Gamma-globulins): Antibodies produced by leukocytes.
Clotting Proteins: Essential for blood clot formation.
Transport Proteins: Carry hydrophobic molecules (e.g., lipids, steroids) through blood.
Cirrhosis and Plasma Protein Deficiency
Cirrhosis (liver disease) leads to decreased plasma protein production, causing edema (ascites) and impaired clotting.

Erythrocytes (Red Blood Cells) and Oxygen Transport
Structure and Function
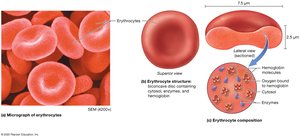
Erythrocytes are biconcave, anucleate cells specialized for gas exchange. They contain hemoglobin, a protein that binds and transports oxygen and carbon dioxide.
Diameter: ~7.5 µm; lack nuclei and most organelles.
Hemoglobin (Hb): Four polypeptide chains (2 alpha, 2 beta), each with an iron-containing heme group.
Oxyhemoglobin: Hb bound to O2 (lungs); Deoxyhemoglobin: Hb without O2 (tissues).
Carbaminohemoglobin: Hb bound to CO2 (tissues).
Carboxyhemoglobin: Hb bound to CO (carbon monoxide); binding is irreversible and toxic.

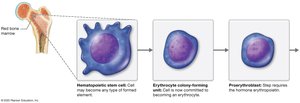
Erythropoiesis (Red Blood Cell Formation)
Erythropoiesis occurs in red bone marrow and is regulated by erythropoietin (EPO) from the kidneys in response to low blood oxygen.
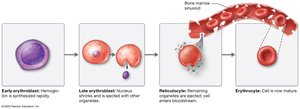
Hematopoietic stem cells → Erythrocyte CFUs → Proerythroblasts → Erythroblasts → Reticulocytes → Erythrocytes
Negative feedback loop maintains hematocrit.

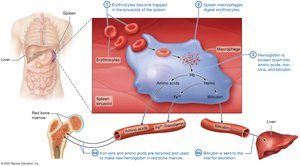
Erythrocyte Lifespan and Destruction
Erythrocytes live 100–120 days. Old cells are removed by macrophages in the spleen and liver. Hemoglobin is broken down and components are recycled or excreted.
Iron is recycled via transferrin.
Bilirubin (from heme) is excreted in bile.
Anemia
Anemia is a decrease in the oxygen-carrying capacity of blood, with symptoms such as pallor, fatigue, and shortness of breath. Causes include:
Decreased Hemoglobin: Iron-deficiency anemia, anemia of chronic disease, vitamin deficiencies.
Decreased Hematocrit: Blood loss, pernicious anemia, hemolytic anemia, aplastic anemia.
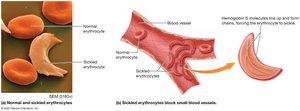
Abnormal Hemoglobin: Sickle-cell disease (HbS), thalassemia.

Complete Blood Count (CBC)
CBC is a laboratory test that measures the number and characteristics of blood cells, including erythrocytes, leukocytes, and platelets. It helps diagnose anemia, infections, and other blood disorders.

Polycythemia
Polycythemia is an elevated hematocrit. It can be primary (bone marrow disorder) or secondary (response to hypoxia, high altitude, or other conditions). Risks include blood clots and increased blood viscosity.
Leukocytes (White Blood Cells) and Immune Function
Classification and Function
Leukocytes are larger than erythrocytes, have nuclei, and are involved in immune defense. They exit the bloodstream to reach tissues.
Granulocytes: Neutrophils, eosinophils, basophils (contain cytoplasmic granules).
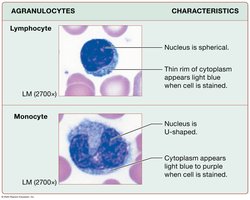
Agranulocytes: Lymphocytes, monocytes (lack specific granules).

Granulocytes
Neutrophils: Most common; phagocytize bacteria; multi-lobed nucleus.
Eosinophils: Respond to parasitic infections and allergies; bilobed nucleus; red granules.
Basophils: Rarest; mediate inflammation; S-shaped nucleus; dark blue granules.
Agranulocytes
Lymphocytes: B cells (produce antibodies), T cells (destroy abnormal cells, activate immune response).
Monocytes: Largest WBCs; become macrophages in tissues; phagocytize debris and activate other leukocytes.
Leukopoiesis (Leukocyte Formation)
Leukocytes arise from hematopoietic stem cells in bone marrow via myeloid and lymphoid cell lines.

Leukemias
Leukemias are cancers of blood cells or bone marrow, classified as acute or chronic, and lymphocytic or myelogenous. They impair normal blood cell production and can metastasize.


Platelets and Hemostasis
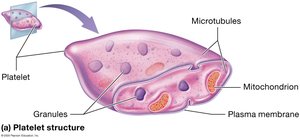
Platelet Structure and Formation
Platelets are cell fragments involved in blood clotting. They are produced from megakaryocytes in the bone marrow, stimulated by thrombopoietin.

Hemostasis: Stopping Blood Loss
Overview of Hemostasis
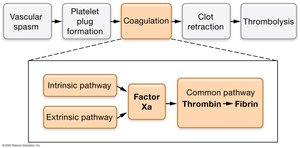
Hemostasis is the process that stops bleeding and involves five steps:
Vascular spasm
Platelet plug formation
Coagulation (clotting)
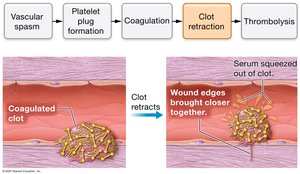
Clot retraction
Thrombolysis (clot dissolution)

Step 1: Vascular Spasm
Injury to a blood vessel causes vasoconstriction and increased tissue pressure, reducing blood flow and loss.


Step 2: Platelet Plug Formation
Platelets adhere to exposed collagen, become activated, and aggregate to form a temporary plug. Von Willebrand factor (vWF) is crucial for platelet activation.

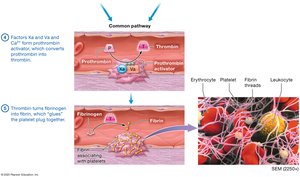
Step 3: Coagulation
Coagulation converts the platelet plug into a stable clot via the coagulation cascade, involving intrinsic and extrinsic pathways that converge on the common pathway to produce fibrin.
Intrinsic Pathway: Triggered by exposed collagen; involves factors XII, XI, IX, VIII.
Extrinsic Pathway: Triggered by tissue factor; involves factor VII.
Common Pathway: Factor X activation leads to thrombin formation, which converts fibrinogen to fibrin.



Step 4: Clot Retraction
Platelet actin and myosin contract, pulling wound edges together and squeezing serum from the clot.
Step 5: Thrombolysis
After healing, the clot is dissolved by plasmin, which degrades fibrin. Tissue plasminogen activator (tPA) initiates this process.

Hemostasis: The Big Picture

Regulation and Disorders of Clotting
Regulation of Clotting
Clotting is regulated by endothelial cell products (prostacyclin, nitric oxide) and anticoagulants (antithrombin, heparan sulfate, protein C).
Clotting Disorders
Bleeding Disorders: Hemophilia A (factor VIII deficiency), Hemophilia B (factor IX deficiency).
Hypercoagulable States: Thrombosis, embolism, deep vein thrombosis (DVT), pulmonary embolism, stroke, myocardial infarction.
Anticlot Medications
Heparin: Immediate action, hospital use.
Warfarin: Oral, inhibits vitamin K-dependent factors.
Direct Factor Xa Inhibitors: Apixaban, rivaroxaban.
Antiplatelet Drugs: Aspirin, clopidogrel, glycoprotein IIb/IIIa inhibitors.


Blood Typing and Transfusions
Blood Groups and Antigens
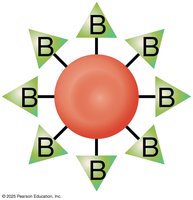
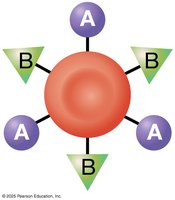
Blood groups are determined by antigens on erythrocytes. The two most important are the ABO and Rh groups.
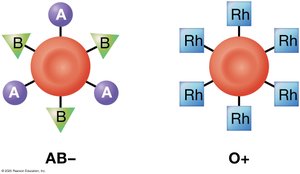
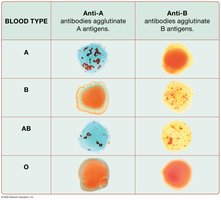
ABO Group: Type A (A antigen), Type B (B antigen), Type AB (A and B antigens), Type O (no antigens).
Rh Group: Rh+ (D antigen present), Rh− (D antigen absent).
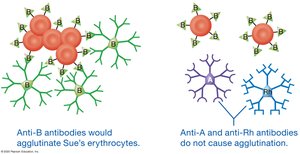
Hemolytic Disease of the Newborn
Occurs when an Rh− mother carries an Rh+ fetus, leading to maternal antibody production and fetal erythrocyte destruction in subsequent pregnancies. Prevented by administering Rh immunoglobulin to the mother.

Blood Typing and Agglutination
Blood type is determined by mixing blood with anti-A, anti-B, and anti-Rh antibodies and observing agglutination (clumping).

Blood Transfusions and Compatibility
Transfusion reactions occur if donor erythrocytes have antigens that the recipient's antibodies recognize as foreign. Type O− is the universal donor; AB+ is the universal recipient.


Donor Antibodies
Donor antibodies are present in small amounts and usually do not cause significant reactions in the recipient, but recipient antibodies can destroy donor erythrocytes if not matched properly.
Additional info: For a comprehensive understanding, students should review the coagulation cascade, the regulation of erythropoiesis, and the clinical implications of blood disorders and transfusion reactions. Practice interpreting CBC results and blood typing charts for exam preparation.
