 Back
BackFluid, Electrolyte, and Acid-Base Balance: Study Notes for Anatomy & Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Fluid & Electrolyte Balance
Body Fluid Volumes
Water is the most abundant compound in the human body, playing a critical role in physiological processes. The distribution and volume of body fluids vary based on age, gender, and body composition.
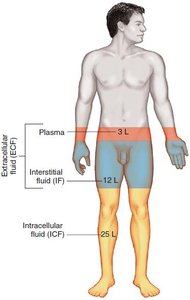
Average body water volume: 40 L in a healthy, nonobese 70-kg male.
Fluid compartments: Plasma (3 L), Interstitial fluid (12 L), Intracellular fluid (25 L).
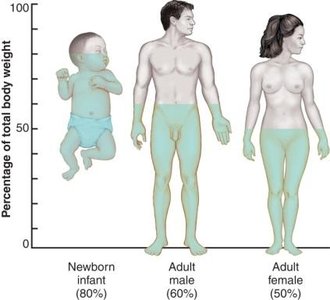
Percentage of body weight: Water is 80% in newborns, 60% in adult males, and 50% in adult females.
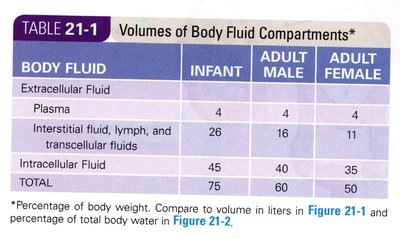
BODY FLUID | INFANT | ADULT MALE | ADULT FEMALE |
|---|---|---|---|
Plasma | 4 | 4 | 4 |
Interstitial fluid, lymph, and transcellular fluids | 26 | 16 | 11 |
Intracellular Fluid | 45 | 40 | 35 |
TOTAL | 75 | 60 | 50 |
Variation in Total Body Water
Total body water content is influenced by several factors:
Body weight: Higher body weight generally means more water, but fat tissue contains less water than muscle.
Fat content: More fat reduces water content per kilogram.
Gender: Females typically have about 10% less water than males.
Age: Water percentage decreases with age due to increased fat and decreased muscle mass.
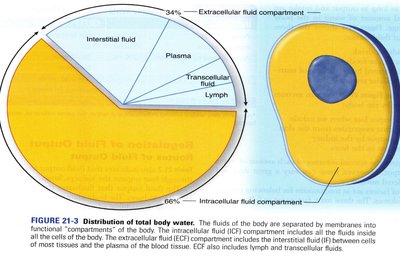
Body Fluid Compartments
Body fluids are divided into compartments:
Extracellular fluid (ECF): Includes plasma, interstitial fluid (IF), lymph, joint fluids, cerebrospinal fluid, and eye humors. ECF surrounds cells and transports substances.
Intracellular fluid (ICF): Largest compartment, located inside cells, facilitating intracellular chemical reactions.
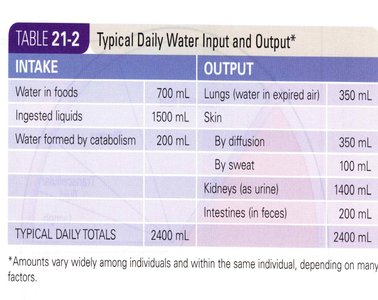
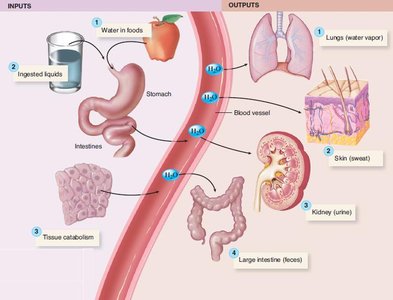
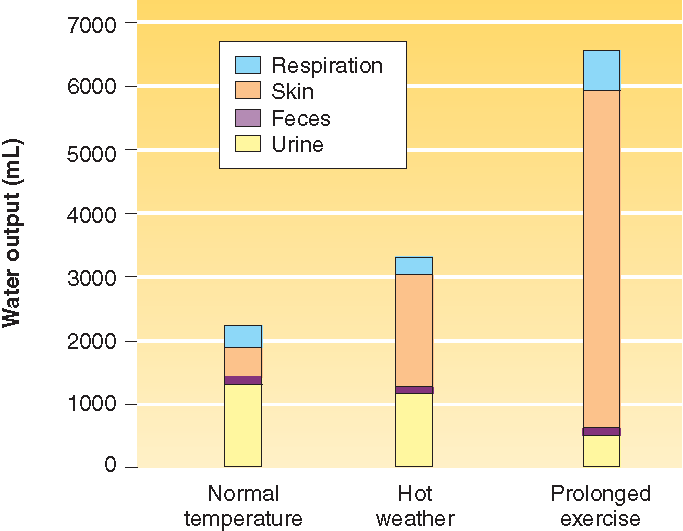
Sources of Fluid Intake and Output
Fluid balance is maintained by matching intake and output:
Intake: Liquids, water in food, metabolic water from cellular respiration.
Output: Water vapor (respiration), sweating, urine, feces.
INTAKE | OUTPUT |
|---|---|
Water in foods: 700 mL | Lungs (expired air): 350 mL |
Ingested liquids: 1500 mL | Skin (diffusion): 350 mL |
Water formed by catabolism: 200 mL | Skin (sweat): 100 mL |
Kidneys (urine): 1400 mL | |
Intestines (feces): 200 mL | |
TOTAL: 2400 mL | TOTAL: 2400 mL |
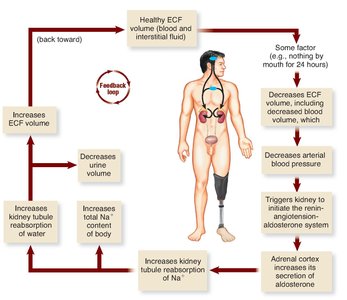
Fluid Balance and Regulation
Fluid balance is achieved by adjusting output, mainly urine volume, to match intake. Several hormones regulate this process:
Antidiuretic hormone (ADH): Released from the posterior pituitary when ECF volume is low; increases kidney reabsorption of water.
Aldosterone: From adrenal cortex; increases sodium and water reabsorption in kidneys.
Atrial natriuretic hormone (ANH): Released from the atrial wall of the heart; increases urine volume by promoting sodium and water loss.
Capillary Blood Pressure and Blood Proteins
Capillary blood pressure and plasma protein concentration influence fluid movement:
Increased capillary blood pressure: Transfers fluid from blood to interstitial fluid (IF).
Blood plasma proteins: Create osmotic pressure, attracting water and holding it in plasma.
Fluid Imbalances
Imbalances can occur when intake and output are not matched:
Dehydration: Total body fluid volume is lower than normal; IF volume shrinks first, followed by ICF and plasma.
Overhydration: Total body fluid volume is higher than normal; excess volume burdens the heart.
Water intoxication: Severe overhydration with electrolyte imbalance, potentially life-threatening.

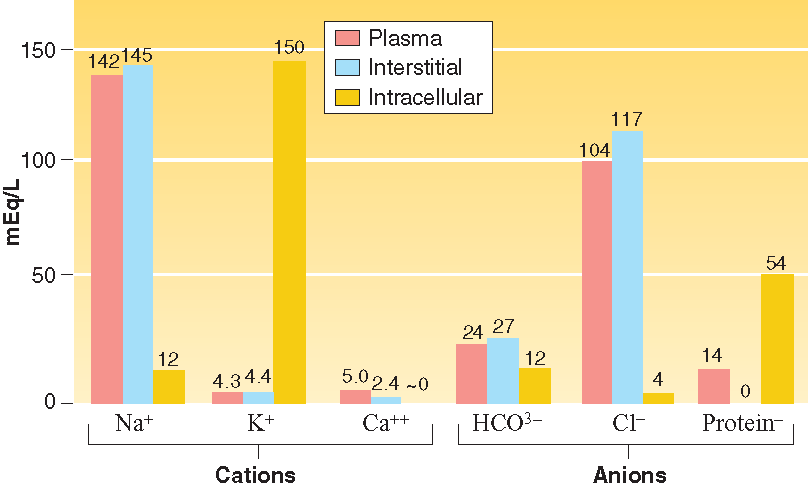
Importance of Electrolytes in Body Fluids
Electrolytes are essential for physiological functions:
Nonelectrolytes: Organic substances that do not dissociate in water (e.g., glucose).
Electrolytes: Compounds that dissociate into ions in water (e.g., sodium chloride).
Ions: Cations (positive, e.g., Na+, K+) and anions (negative, e.g., Cl-, HCO3-).
Electrolyte | Imbalance | Blood Concentration | Possible Outcomes |
|---|---|---|---|
Sodium (Na+) | Hypernatremia | >145 mEq/L | Headache, confusion, seizures |
Sodium (Na+) | Hyponatremia | <136 mEq/L | Headache, confusion, seizures; coma and death in severe cases |
Potassium (K+) | Hyperkalemia | >5.1 mEq/L | Weakening and paralysis of skeletal muscle |
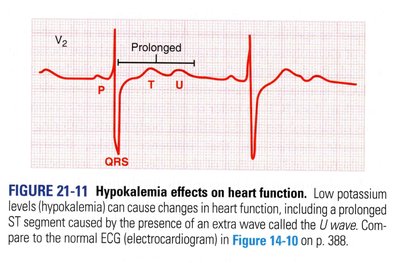
Potassium (K+) | Hypokalemia | <3.5 mEq/L | Cardiac dysrhythmia or arrest; GI motility problems |
Calcium (Ca++) | Hypercalcemia | >5.26 mEq/L | Fatigue, muscle weakness, diminished reflexes, impaired cardiac conduction |
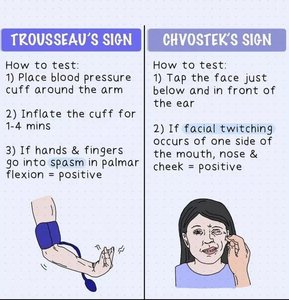
Calcium (Ca++) | Hypocalcemia | <4.2 mEq/L | Muscle cramping and twitching, hyperactive reflexes, cardiac dysrhythmia |
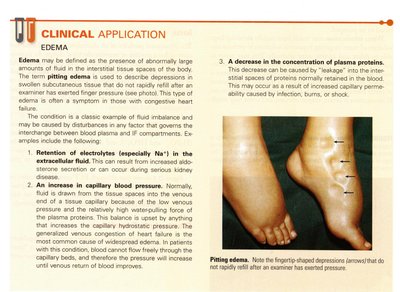
Clinical Application: Edema
Edema is the presence of abnormally large amounts of fluid in interstitial spaces. Pitting edema is identified by depressions in swollen tissue that do not rapidly refill after pressure is applied.
Causes: Retention of electrolytes (especially Na+), increased capillary blood pressure, decreased plasma protein concentration.

Electrolyte Imbalances
Disruptions in electrolyte homeostasis can lead to various clinical conditions:
Hypernatremia: Blood sodium >145 mEq/L; causes include overuse of salt tablets, dehydration, prolonged diarrhea.
Hyponatremia: Blood sodium <136 mEq/L; causes include excessive ADH secretion, sodium-free IV infusion, burns, diuretics.
Hyperkalemia: Blood potassium >5.1 mEq/L; causes include increased intake, tissue trauma, renal failure.
Hypokalemia: Blood potassium <3.5 mEq/L; causes include fasting, low-potassium diets, laxative abuse, diarrhea, vomiting.
Hypercalcemia: Blood calcium >10.5 mg/dL; causes include excessive input, increased absorption, bone disease, hyperparathyroidism.
Hypocalcemia: Blood calcium <8.4 mg/dL; causes include dietary deficiency, decreased absorption, increased excretion, hypoparathyroidism.
Review Questions & Quick Checks
Electrolytes: Substances that dissociate in water to form ions.
Fluid compartments: Extracellular and intracellular.
Factors affecting fluid volumes: Capillary blood pressure, protein concentration, fat content, age, gender.
Pitting edema: Depressions in swollen tissue that do not rapidly refill.
Water movement: Largely depends on capillary blood pressure and plasma protein concentration.
Hypernatremia: Overuse of salt tablets, dehydration, prolonged diarrhea.
Hypercalcemia: Decreased neuromuscular irritability, fatigue, muscle weakness, diminished reflexes.
Additional info:
Electrolyte balance is crucial for nerve conduction, muscle contraction, and maintaining osmotic pressure.
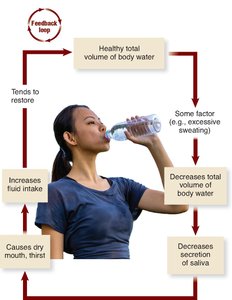
Fluid balance is regulated by feedback mechanisms involving thirst and hormone release.
Clinical signs of electrolyte imbalances often involve neurological and muscular symptoms.
