 Back
BackMetabolism and Regulation of Body Temperature: Liver, Lipoproteins, Thyroid Hormones, and Appetite Control
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Metabolism and the Liver
General Metabolic Functions of the Liver
The liver is the central metabolic organ of the body, responsible for processing nutrients, regulating plasma cholesterol, and detoxifying substances. Hepatocytes, the main liver cells, perform a wide range of biochemical reactions essential for homeostasis.
Fatty Acid Processing: Packages free fatty acids (FFA) into forms for storage or transport.
Protein Synthesis: Synthesizes plasma proteins such as albumin and clotting factors.
Amino Acid Metabolism: Forms nonessential amino acids, deaminates amino acids, and converts ammonia to urea for excretion.
Glucose Storage and Regulation: Stores glucose as glycogen and is a key site for gluconeogenesis (formation of glucose from non-carbohydrate sources).
Vitamin and Mineral Storage: Stores vitamins A, D, B12, and iron (as ferritin).
Hormone and Drug Metabolism: Degrades hormones and metabolizes toxic substances such as alcohol and drugs.
Lipoproteins and Cholesterol Transport
Types and Functions of Lipoproteins
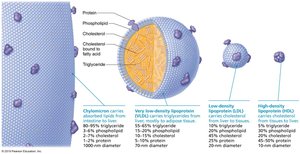
Lipoproteins are complexes that transport triglycerides and cholesterol in the blood. Their density depends on the ratio of lipid to protein: the higher the lipid content, the lower the density.
Type | Lipid/Protein (%) | Function |
|---|---|---|
Chylomicrons | ~99/1 | Transport dietary lipids from intestine to tissues |
VLDLs | ~92/8 | Transport triglycerides from liver to adipose tissue |
LDLs | ~75/25 | Deliver cholesterol to tissues |
HDLs | ~50/50 | Transport cholesterol from tissues to liver for excretion |
HDLs are considered "good" because they remove cholesterol from tissues for degradation. LDLs are "bad" because excess LDLs can deposit cholesterol in blood vessel walls, increasing cardiovascular risk.

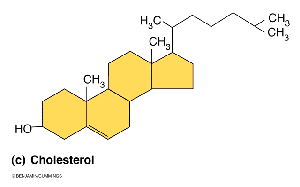
Dietary Fats and Cholesterol Levels
Saturated Fatty Acids: Stimulate cholesterol synthesis and inhibit its excretion.
Unsaturated Fatty Acids: Enhance cholesterol excretion via bile salts.
Trans Fats: Increase LDL production and elevate blood cholesterol levels more than saturated fats.
A healthy cholesterol level is below 200 mg/dL, but the ratio of saturated to unsaturated fats in the diet is more important than total cholesterol intake.
Thyroid Hormone and Metabolic Rate
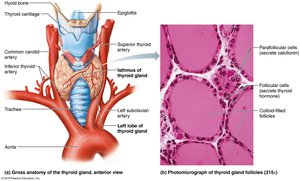
Thyroid Gland Structure and Hormone Synthesis
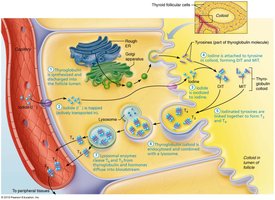
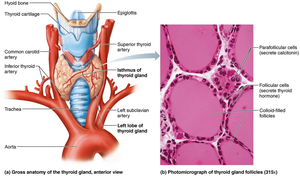
The thyroid gland, located on the trachea below the larynx, is the largest pure endocrine gland. It consists of colloid-filled follicles surrounded by follicular cells (produce thyroglobulin, the precursor to thyroid hormones) and parafollicular cells (produce calcitonin).
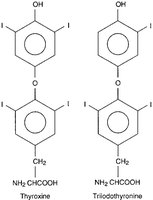
Thyroid Hormones: T3 and T4
The thyroid produces two iodine-containing hormones:
Thyroxine (T4): Main product, less active, converted to T3 in target tissues.
Triiodothyronine (T3): More active, binds more avidly to receptors, about 10 times more potent than T4.
Synthesis of Thyroid Hormone
Thyroid hormone synthesis involves iodination of tyrosine residues in thyroglobulin, followed by coupling to form T3 and T4, which are stored in the colloid and released upon stimulation by TSH.
Functions of Thyroid Hormones
Increase Basal Metabolic Rate (BMR): Stimulate glucose oxidation and heat production (calorigenic effect).
Regulate Blood Pressure: Increase adrenergic receptors in blood vessels.
Promote Growth and Development: Essential for normal skeletal and nervous system development, especially in fetus and infants.
Maintain Tissue Function: Important for adult tissue maintenance and reproductive function.
Regulation of Thyroid Hormone Secretion
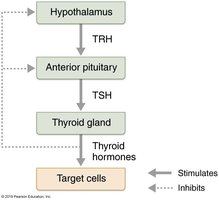
Thyroid hormone secretion is controlled by a three-tiered negative feedback system involving the hypothalamus (TRH), anterior pituitary (TSH), and thyroid gland (T3 and T4). T3 is more active due to higher receptor affinity and is the main effector at target tissues.
Thyroid Disorders
Hypothyroidism
In Adults: Causes include autoimmune thyroiditis (e.g., Hashimoto’s disease), TSH/TRH deficits, iodine deficiency, or thyroidectomy. Symptoms: low BMR, cold intolerance, constipation, dry skin, puffy eyes, edema, lethargy, and mental sluggishness.
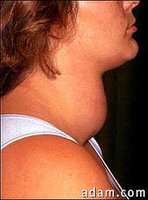
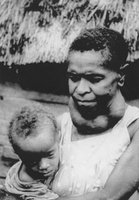
Goiter: Due to iodine deficiency; thyroid cannot produce T3/T4, but TSH continues to stimulate gland, causing enlargement. Reversible with iodine supplementation.
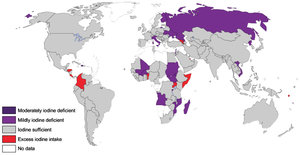
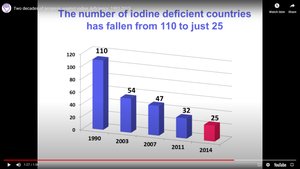
Global Iodine Deficiency
Iodine deficiency is less common due to salt iodization, but still exists in some regions. The Iodine Global Network tracks and promotes iodine sufficiency worldwide.
Congenital Iodine Deficiency Syndrome
In fetuses and infants, thyroid hormone deficiency leads to impaired nervous and skeletal development, resulting in intellectual disability and growth abnormalities. Early hormone therapy can partially reverse effects.
Hyperthyroidism
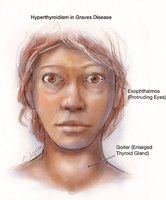
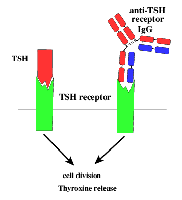
Grave’s Disease: Autoimmune disorder where antibodies mimic TSH, causing continuous thyroid stimulation. Symptoms: high BMR, sweating, rapid heartbeat, nervousness, weight loss, exophthalmos, and goiter. Treatment includes thyroid removal or radioactive iodine.
Calcitonin
Calcitonin is a polypeptide hormone from parafollicular cells of the thyroid. It lowers blood calcium by inhibiting bone resorption and stimulating calcium uptake into bone. Its role is most significant during childhood.
Metabolic Rate and Its Regulation
Basal Metabolic Rate (BMR) and Total Metabolic Rate (TMR)
Metabolic rate is the rate of energy expenditure by the body. BMR is measured under basal conditions (rest, fasting, thermoneutral environment) and reflects the energy cost of living. TMR includes BMR plus energy used for voluntary activities and digestion.
BMR Influences: Surface area, age, gender, stress, and hormones (especially thyroid hormone).
Thyroid Hormone: Increases oxygen consumption and ATP use, raising BMR. Hyperthyroidism increases BMR; hypothyroidism decreases it.
Other Factors: Stress (via norepinephrine/epinephrine), fever, and physical activity can also raise metabolic rate.
Regulation of Appetite and Energy Balance
Energy Intake, Output, and Storage
Energy balance is achieved when energy intake equals energy output (heat, work, and storage). Excess energy is stored as fat or glycogen. Body mass index (BMI) is used to assess weight status, but does not distinguish between muscle and fat mass.
Appetite, Hunger, and Satiety
Appetite is the desire for food, influenced by memory, emotions, and environment. Hunger is a physiological need for food, while satiety is the satisfaction of hunger. Eating behavior is regulated by neural signals, hormones, and nutrient levels.

Neural and Hormonal Regulation of Appetite
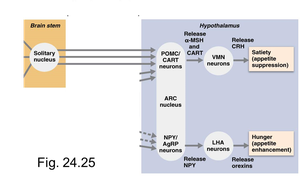
Hunger Promotion: Arcuate nucleus neurons release neuropeptide Y (NPY) and agouti-related peptide (AgRP), stimulating the lateral hypothalamic area (LHA) to release orexins, which enhance hunger.
Satiety Promotion: POMC/CART neurons release α-MSH and CART, acting on the ventromedial nucleus (VMN) to release CRH, suppressing appetite.
Short-Term and Long-Term Signals
Short-Term: Neural signals from GI tract (stretch receptors), nutrient signals (protein, carbohydrates), and hormones (insulin, cholecystokinin, glucagon, epinephrine, ghrelin) regulate hunger and satiety.
Long-Term: Leptin from adipose tissue signals fat stores, decreasing hunger and increasing satiety. However, leptin resistance can occur in obesity.


Other Factors Affecting Appetite
Body Temperature: Increased temperature may depress hunger; cold climates may stimulate eating.
Psychological Factors: Emotional state and learned behaviors can influence eating patterns.
Gut Microbiota: Bacteria in the large intestine can release peptides that affect appetite regulation.
Note: There is no simple answer to appetite regulation; it is a complex interplay of neural, hormonal, and environmental factors.
