 Back
BackMuscle Tissue: Structure, Function, and Types
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Muscle Tissue Overview
Introduction to Muscle Tissue
Muscle tissue is a specialized tissue found throughout the human body, responsible for producing movement by contracting and relaxing. It constitutes nearly half of the body's mass and transforms chemical energy (ATP) into mechanical energy, enabling force generation and movement.
Three types of muscle tissue: Skeletal, Cardiac, and Smooth
Main functions: Movement, posture maintenance, joint stabilization, and heat generation
Types of Muscle Tissue
Skeletal Muscle
Skeletal muscle is attached to bones and skin, allowing voluntary movements. Its cells are elongated, multinucleated, and striated. Skeletal muscle contracts rapidly but tires easily and requires nervous system stimulation.
Location: Attached to bones or skin
Control: Voluntary (conscious control)
Structure: Long, cylindrical, multinucleate cells with striations
Cardiac Muscle
Cardiac muscle is found only in the heart, forming the bulk of the heart walls. It is striated like skeletal muscle but is involuntary and can contract without nervous system stimulation.
Location: Walls of the heart
Control: Involuntary
Structure: Branching chains of cells, uni- or binucleate, striated
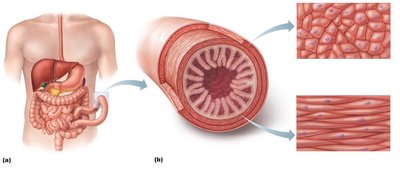
Smooth Muscle
Smooth muscle is located in the walls of hollow organs (except the heart), such as the stomach, urinary bladder, and airways. It is not striated and contracts involuntarily, often in response to local chemical or neural stimuli.
Location: Walls of hollow organs
Control: Involuntary
Structure: Single, fusiform, uninucleate cells without striations
Comparison of Muscle Tissue Types
Structural and Functional Differences
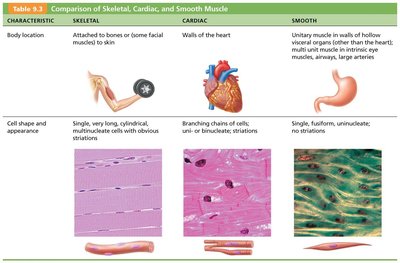
The three muscle types differ in structure, control, and function. The following table summarizes key differences:
Characteristic | Skeletal | Cardiac | Smooth |
|---|---|---|---|
Body location | Attached to bones or skin | Walls of the heart | Walls of hollow organs (except heart) |
Cell shape & appearance | Long, cylindrical, multinucleate, striated | Branching, uni- or binucleate, striated | Single, fusiform, uninucleate, no striations |
Control | Voluntary | Involuntary | Involuntary |
Special Characteristics of Muscle Tissue
Excitability: Ability to receive and respond to stimuli
Contractility: Ability to shorten forcibly when stimulated
Extensibility: Ability to be stretched
Elasticity: Ability to recoil to resting length
Functions of Muscle Tissue
Movement of bones or fluids
Maintaining posture and body position
Stabilizing joints
Heat generation (especially skeletal muscle)
Additional: Protects organs, forms valves, controls pupil size, causes "goosebumps"
Structure and Organization of Skeletal Muscle
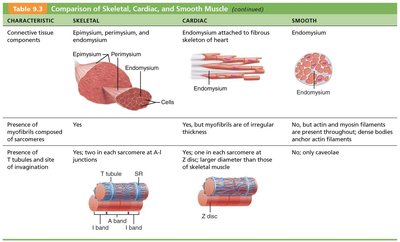
Connective Tissue Sheaths
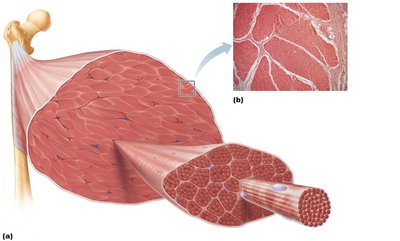
Skeletal muscle is organized into several layers of connective tissue sheaths that support and reinforce the muscle:
Epimysium: Surrounds the entire muscle
Perimysium: Surrounds fascicles (bundles of muscle fibers)
Endomysium: Surrounds each individual muscle fiber
Levels of Organization
Structure | Description | Connective Tissue Wrapping |
|---|---|---|
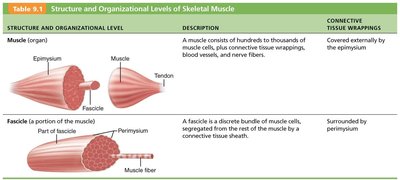
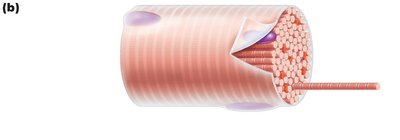
Muscle (organ) | Hundreds to thousands of muscle cells, connective tissue, blood vessels, nerve fibers | Epimysium |
Fascicle | Discrete bundle of muscle cells | Perimysium |
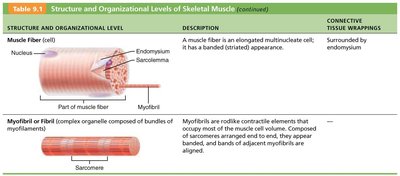
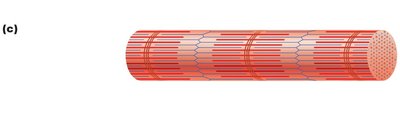
Muscle fiber (cell) | Elongated, multinucleate cell with striations | Endomysium |
Myofibril | Rodlike contractile element, most of cell volume, composed of sarcomeres | — |
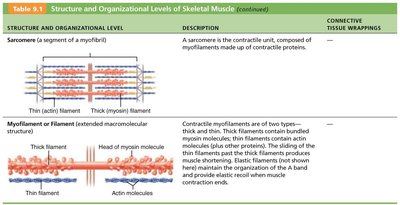
Sarcomere | Contractile unit, composed of myofilaments | — |
Myofilament | Thick (myosin) and thin (actin) filaments | — |
Microscopic Anatomy of Skeletal Muscle
Myofibrils and Sarcomeres
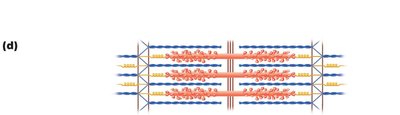
Myofibrils are densely packed, rodlike elements that make up about 80% of the muscle cell volume. They contain repeating units called sarcomeres, which are the functional contractile units of muscle fibers. Sarcomeres are composed of thick (myosin) and thin (actin) filaments, responsible for the striated appearance of skeletal muscle.
Striations: Alternating dark A bands and light I bands
H zone: Lighter region in the middle of the A band
M line: Line of protein myomesin bisecting the H zone
Z disc: Sheet of proteins anchoring thin filaments and connecting myofibrils
Interaction of Thick and Thin Filaments
The interaction between actin (thin) and myosin (thick) filaments within the sarcomere is responsible for muscle contraction. Myosin heads form cross-bridges with actin filaments, pulling them toward the center of the sarcomere during contraction.
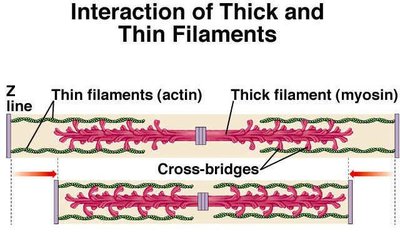
Muscle Contraction: The Sliding Filament Model
During contraction, thin filaments slide past thick filaments, increasing their overlap. This process shortens the sarcomere and, consequently, the entire muscle fiber. The sliding filament model explains how muscle fibers contract to produce force.
Key events: Myosin heads attach to actin, forming cross-bridges, and pull thin filaments toward the center
Result: I bands shorten, Z discs move closer, H zones disappear, A bands move closer but do not change length
Physiology of Skeletal Muscle Contraction
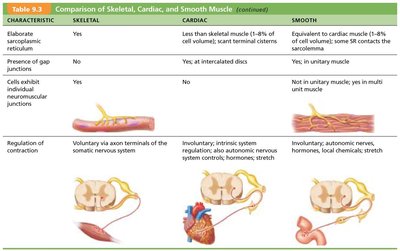
Activation and Excitation-Contraction Coupling
Activation: Nervous system stimulates muscle fibers at the neuromuscular junction, generating an action potential in the sarcolemma
Excitation-Contraction Coupling: Action potential propagates along the sarcolemma, leading to a brief rise in intracellular Ca2+ levels, which triggers contraction
Destruction of Acetylcholine
Acetylcholine (ACh) is released at the neuromuscular junction to initiate contraction. Its effects are quickly terminated by acetylcholinesterase, preventing continuous muscle contraction in the absence of further stimulation.
Muscle Tone
Muscle tone is the constant, slightly contracted state of all muscles, maintained by spinal reflexes. It keeps muscles firm, healthy, and ready to respond to stimuli.
Energy Systems in Muscle Activity
ATP Sources During Exercise
Muscle contraction requires ATP, which is supplied by different energy systems depending on the duration and intensity of activity:
Immediate: ATP stored in muscles (used for a few seconds)
Short-term: ATP generated from creatine phosphate and ADP (direct phosphorylation, up to 10 seconds)
Intermediate: Glycogen breakdown to glucose (anaerobic pathway, 30–40 seconds)
Long-term: ATP generated by aerobic metabolism (prolonged exercise)
Muscle Fatigue and Recovery
Muscle fatigue: Inability to contract despite continued stimulation, often due to ionic imbalances or damage to the sarcoplasmic reticulum
Recovery: Excess postexercise oxygen consumption (EPOC) restores muscle to resting state by replenishing oxygen, converting lactic acid, and restoring ATP and creatine phosphate reserves
Smooth Muscle Structure and Function
Organization and Microscopic Structure
Smooth muscle is found in the walls of most hollow organs, usually arranged in two layers (longitudinal and circular). Its fibers are spindle-shaped, uninucleate, and lack striations. Smooth muscle contracts in a slow, synchronized manner and can maintain contraction for prolonged periods with little energy cost.
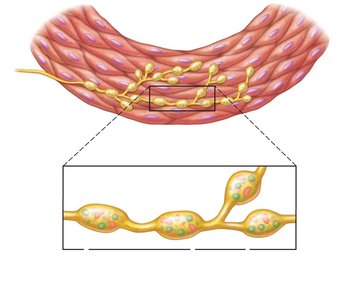
Innervation and Contraction
Innervation: Autonomic nerve fibers innervate smooth muscle at diffuse junctions via varicosities, releasing neurotransmitters
Contraction: Actin and myosin interact by the sliding filament mechanism; contraction is regulated by nerves, hormones, or local chemical changes
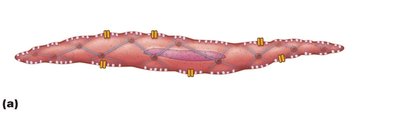
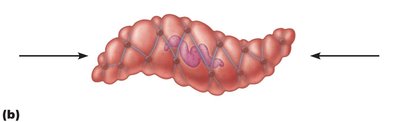
Special Features of Smooth Muscle
Stress-relaxation response: Smooth muscle adapts to stretch and can contract on demand
Length and tension changes: Can contract when between half and twice its resting length
Hyperplasia: Smooth muscle cells can divide and increase in number (e.g., uterus during pregnancy)
Types of Smooth Muscle
Unitary (visceral) smooth muscle: In hollow organs (except heart), arranged in sheets, electrically coupled by gap junctions, often spontaneously active
Multiunit smooth muscle: In large airways, arteries, arrector pili, and iris; independent fibers, innervated by autonomic nervous system, graded contractions
Muscular Dystrophy
Overview
Muscular dystrophy is a group of inherited diseases characterized by progressive muscle degeneration and weakness. The most common type is Duchenne muscular dystrophy (DMD), caused by a lack of dystrophin, a protein that stabilizes the sarcolemma.
Symptoms: Muscle enlargement due to fat and connective tissue deposits, muscle fiber atrophy, clumsiness, frequent falls
Progression: Loss of muscle regenerative capacity, respiratory failure in early adulthood
Treatments: No cure; prednisone, gene therapy, and stem cell infusion show promise
