 Back
BackRepro 5 -March 30
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Reproduction and Development
Hormonal Control of the Menstrual Cycle
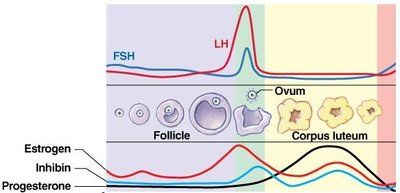
The menstrual cycle is regulated by a complex interplay of hormones from the hypothalamus, pituitary gland, and ovaries. These hormones coordinate the development of ovarian follicles, ovulation, and preparation of the endometrium for possible pregnancy.
Follicle-Stimulating Hormone (FSH) and Luteinizing Hormone (LH) are released from the anterior pituitary in response to Gonadotropin-Releasing Hormone (GnRH) from the hypothalamus.
Estrogen is produced by developing follicles and is responsible for the proliferation of the endometrial lining.
Progesterone is secreted by the corpus luteum after ovulation and maintains the endometrium in a secretory state.
Negative feedback from estrogen and progesterone regulates FSH and LH secretion.
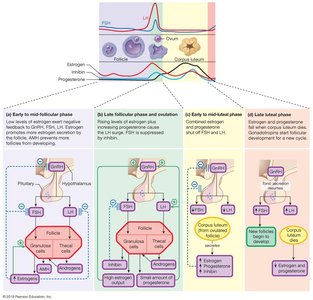
Early to Mid-Luteal Phase
During this phase, the corpus luteum forms from the remnants of the ovulated follicle and secretes high levels of progesterone and estrogen, which inhibit FSH and LH secretion.
Progesterone prepares the endometrium for implantation and forms a cervical mucus plug to prevent infection.
Estrogen and progesterone maintain the endometrial lining.

Late Luteal Phase and Menstruation
If pregnancy does not occur, the corpus luteum degenerates, leading to a drop in estrogen and progesterone. This triggers menstruation and the start of a new cycle.
FSH and LH levels rise as negative feedback is removed.
Endometrial blood vessels constrict, causing tissue breakdown and menstrual bleeding.

Secondary Sex Characteristics in Females
Secondary sex characteristics are physical traits that distinguish the sexes but are not directly involved in reproduction. In females, these are primarily influenced by estrogen and androgens.
Estrogen promotes breast development and the distribution of body fat to hips and thighs.
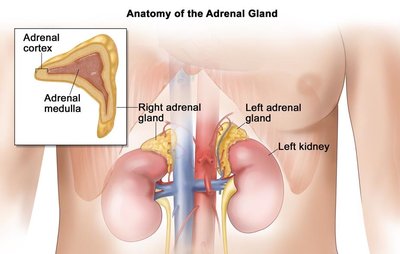
Androgens (from the adrenal cortex) stimulate pubic and axillary hair growth and contribute to libido.

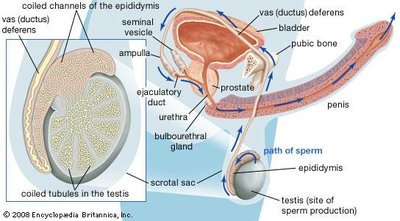
Procreation and the Erection Reflex
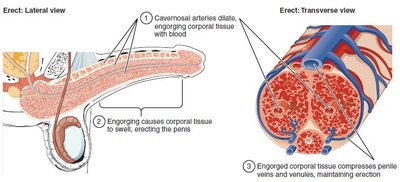
Procreation in humans involves coordinated physiological and behavioral responses to ensure the meeting of egg and sperm. The erection reflex is essential for successful copulation in males.
The penis must become erect (engorged with blood) to allow for sperm deposition in the female reproductive tract.
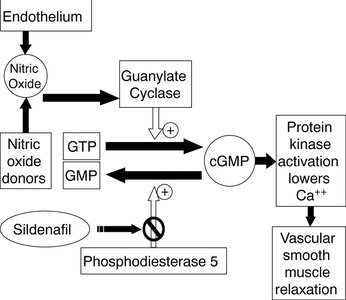
The erection reflex is mediated by parasympathetic nerves, which release acetylcholine (ACh) and stimulate nitric oxide (NO) production, leading to smooth muscle relaxation and increased blood flow.

Emission and Ejaculation
Emission is the movement of sperm and glandular secretions into the urethra, while ejaculation is the forceful expulsion of semen from the body. These processes are controlled by the sympathetic and somatic nervous systems, respectively.
Emission: Sympathetic control moves sperm into the urethra.
Ejaculation: Somatic motor neurons trigger rhythmic contractions to expel semen.
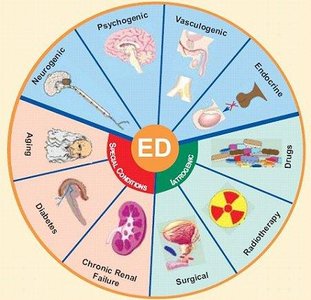
Sexual Dysfunction
Sexual dysfunction can affect both males and females, with erectile dysfunction (ED) being a common issue in men. ED is the inability to achieve or maintain an erection sufficient for intercourse.
Causes include vascular, neurological, endocrine, and psychological factors, as well as certain medications and chronic diseases (e.g., diabetes, cardiovascular disease).
Treatment options include phosphodiesterase type 5 (PDE5) inhibitors such as sildenafil (Viagra), which enhance the effects of nitric oxide and increase blood flow to the penis.
Female Sexual Dysfunction
Female sexual dysfunction often presents as low sexual desire. Treatments include medications that target brain pathways involved in sexual motivation and response, such as flibanserin and bremelanotide.
Androgen therapy may also be used in some cases.
Contraception
Contraceptive methods are designed to prevent pregnancy by inhibiting ovulation, fertilization, or implantation. They are classified into three main categories: abstinence, sterilization, and interventional methods.
Abstinence: Complete avoidance of sexual intercourse.
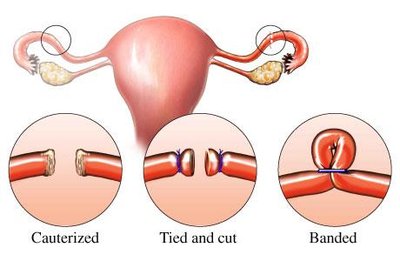
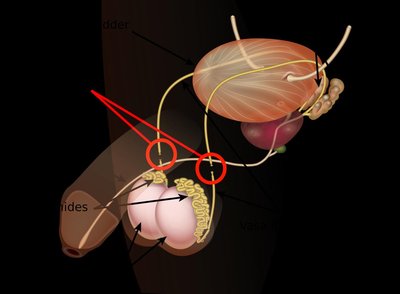
Sterilization: Surgical procedures such as tubal ligation (females) or vasectomy (males) that permanently prevent gamete transport.
Interventional Methods: Include barrier methods, implantation prevention, and hormonal treatments.
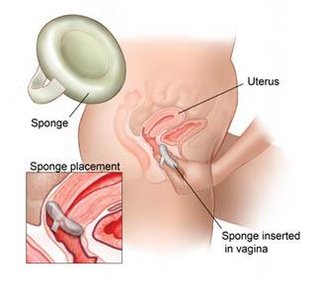
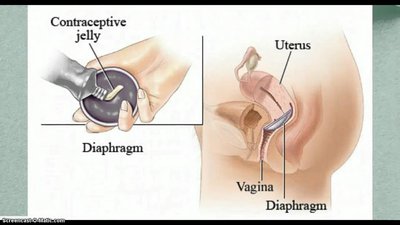
Barrier Methods
Barrier methods physically prevent sperm from reaching the egg. Examples include condoms, diaphragms, cervical caps, and contraceptive sponges.
Effectiveness varies depending on correct and consistent use.
Implantation Prevention
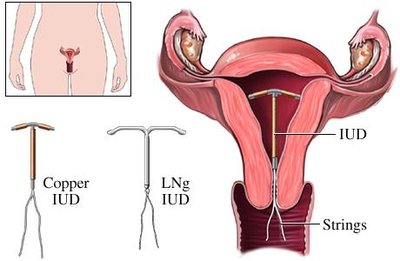
Some contraceptives prevent the implantation of a fertilized egg in the uterus. Intrauterine devices (IUDs) are the most common example, creating a local inflammatory response that is toxic to sperm and ova.
IUDs may be copper-based or hormone-releasing.
Side effects can include pain, bleeding, and risk of pelvic inflammatory disease.
Hormonal Treatments
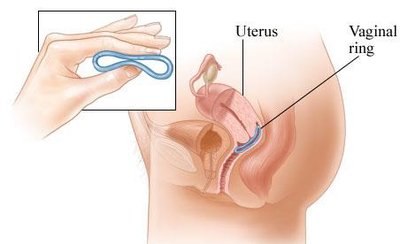
Hormonal contraceptives use synthetic estrogen and/or progestins to inhibit gonadotropin secretion, preventing ovulation and thickening cervical mucus to block sperm entry.
Forms include oral contraceptive pills, injections, implants, patches, and vaginal rings.

Male Contraceptives in Development
Research is ongoing into reversible male contraceptives, including hormone-based regimens and physical barriers such as RISUG/VasalGel, which block sperm transport in the vas deferens.
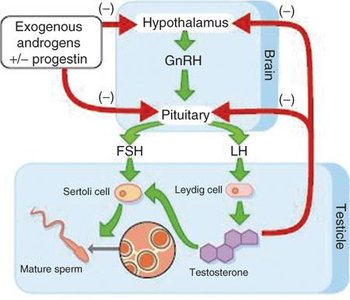
Combination progestin/androgen therapy can suppress spermatogenesis.
Vaccines and novel drugs targeting sperm or testicular function are under investigation.
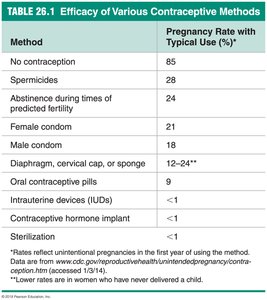
Efficacy of Contraceptive Methods
The effectiveness of contraceptive methods varies widely. The table below summarizes typical pregnancy rates for various methods.
Method | Pregnancy Rate with Typical Use (%) |
|---|---|
No contraception | 85 |
Spermicides | 28 |
Abstinence during times of predicted fertility | 24 |
Female condom | 21 |
Male condom | 18 |
Diaphragm, cervical cap, or sponge | 12–24 |
Oral contraceptive pills | 9 |
Intrauterine devices (IUDs) | <1 |
Contraceptive hormone implant | <1 |
Sterilization | <1 |
Additional info: The menstrual cycle is typically 28 days, with ovulation occurring around day 14. Hormonal contraceptives are among the most effective reversible methods. Male contraceptive options are currently limited but are an active area of research.
