 Back
BackSex Differences in Cardiovascular Disease: Mechanisms, Outcomes, and Clinical Implications
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Sex Differences in Cardiovascular Disease (CVD)
Introduction to Sex and Gender in CVD Research
Understanding the impact of biological sex and gender on cardiovascular disease (CVD) is essential for accurate diagnosis, treatment, and prevention. Most research has historically focused on sex as a biological variable, but emerging studies highlight the importance of considering both sex and gender, especially in transgender and gender-diverse populations.
Sex refers to biological differences (chromosomes, hormones, anatomy).
Gender refers to social and cultural roles, behaviors, and identities.
Both sex and gender influence CVD risk, presentation, and outcomes.
Impact of Sex on Cardiovascular Disease
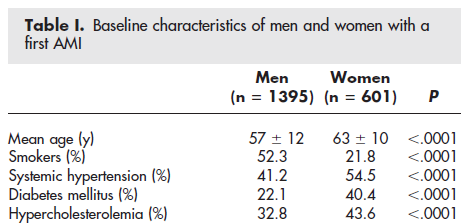
Prevalence and Mortality
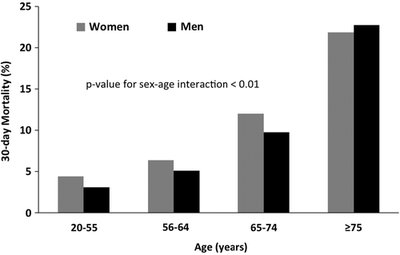
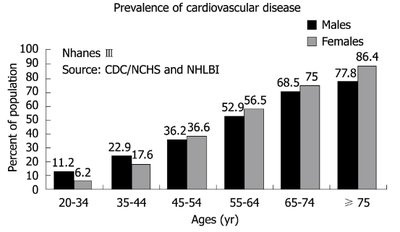
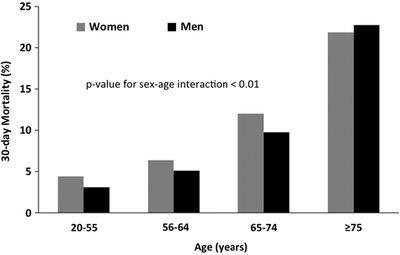
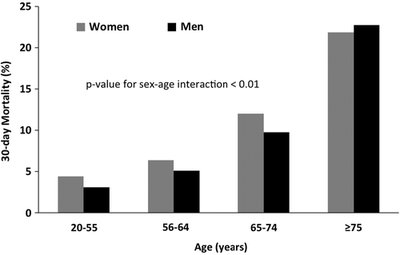
Sex differences are evident in the prevalence and mortality rates of CVD. Women and men exhibit distinct patterns across age groups, with women often experiencing higher mortality at older ages.
Prevalence of CVD increases with age in both sexes, but women surpass men in older age groups.
30-day mortality after acute myocardial infarction (AMI) is higher in women, especially in older age groups.
Symptoms and Clinical Presentation
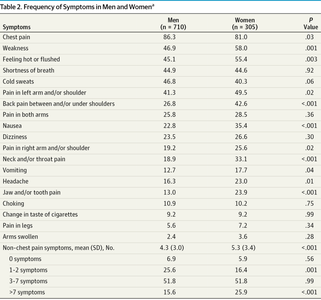
Women and men often present with different symptoms during acute coronary events. Women are less likely to report classic chest pain and more likely to experience atypical symptoms, which can delay diagnosis and treatment.
Women report more symptoms such as weakness, nausea, and shortness of breath.
Men are more likely to present with chest pain and left arm pain.
Non-traditional symptom presentation in women is associated with increased mortality.
Symptom | Men (%) | Women (%) |
|---|---|---|
Chest pain | 86.3 | 81.0 |
Weakness | 46.9 | 58.0 |
Shortness of breath | 44.9 | 44.5 |
Nausea | 23.8 | 36.4 |
Dizziness | 23.5 | 25.6 |
Headache | 10.7 | 17.7 |
Jaw and/or tooth pain | 10.9 | 10.2 |
Arm swelling | 2.4 | 3.6 |
Mechanisms Underlying Sex Differences
Several biological and psychosocial mechanisms contribute to sex differences in CVD outcomes:
Microvascular dysfunction and plaque erosion are more common in women, while men more often experience plaque rupture.
Central pain processing and autonomic/sensory integration differ by sex, influencing symptom perception.
Comorbidities such as diabetes and depression are more prevalent in women with CVD.
Delays in Care and Treatment Disparities
Delay in Seeking Care
Both men and women often delay seeking medical attention for acute cardiac symptoms, but women tend to present later than men. Factors influencing delay include socioeconomic status, knowledge of symptoms, and presence of chronic conditions.
Women report seeking care approximately 30 minutes later than men on average.
Low socioeconomic status and lack of knowledge about AMI increase delays.
Delay in Receiving Treatment
After arrival at the hospital, delays in care delivery are influenced by triage practices and hospital caseload. Women are less likely to receive high-acuity triage scores, especially in high-volume emergency departments.
Arrival by ambulance and presence of cardiac comorbidities increase likelihood of appropriate triage.
Male sex is associated with higher triage priority.
Triage Score | Recommended Time to Physician | Example Presentation | Sentinel Diagnosis |
|---|---|---|---|
1 | Immediate | Code arrest, major shock | AMI with complications |
2 | 15 minutes | Nontraumatic visceral chest pain | AMI, CHF |
3 | 30 minutes | Overdose, GI bleed | Unspecified chest pain |
4 | 60 minutes | Minor trauma, MSK pain | Chest pain not otherwise specified |
5 | 120 minutes | Sore throat, abrasion | Overuse syndrome |
Treatment Disparities
Women are less likely to receive guideline-recommended therapies and invasive procedures compared to men, particularly at younger ages and with less severe disease. These disparities contribute to differences in outcomes.
Lower rates of aspirin, β-blockers, cardiac catheterization, PCI, and CABG in women.
Timeliness of reperfusion (door-to-needle and door-to-balloon times) is lower in women.
Medication prescriptions (antiplatelet agents, statins) are less frequent in women across age groups.
Measure/Treatment | Overall (%) | Men (%) | Women (%) |
|---|---|---|---|
Aspirin within 24h | 92.4 | 93.3 | 91.0 |
β-Blockers within 24h | 86.2 | 87.2 | 84.7 |
Cardiac catheterization | 52.1 | 56.2 | 45.6 |
PCI | 45.9 | 52.3 | 36.1 |
CABG | 7.7 | 9.2 | 5.4 |
Summary of Sex-Dependent Outcomes in CVD
Sex differences in cardiovascular disease are multifactorial, involving biological, clinical, and social determinants. Women experience higher mortality and different symptom profiles, are more likely to have delays in care, and receive less aggressive treatment compared to men. Understanding these differences is critical for improving outcomes and ensuring equitable care.
Explain the sex-dependent differences in CVD outcomes.
Discuss factors involved and the extent of their impact.
