 Back
BackSleep Disorders: Insomnia, Sleep Hygiene, and Pharmacological & Nonpharmacological Management
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Sleep Disorders and the Sleep Cycle
Introduction to Sleep Disorders
Sleep disorders, particularly insomnia, are common conditions that can significantly impact physical and mental health. Understanding the types, causes, and treatments of sleep disorders is essential for effective management and patient counseling.
Insomnia is characterized by difficulty falling asleep, staying asleep, or experiencing non-restorative sleep.
Sleep disorders can be primary or secondary to other medical, psychiatric, or substance-related conditions.
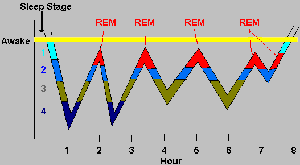
The Sleep Cycle
The sleep cycle consists of several stages, including non-REM (NREM) and REM (rapid eye movement) sleep, which repeat throughout the night.
NREM Sleep: Divided into stages 1-4, with increasing depth of sleep.
REM Sleep: Characterized by rapid eye movements, dreaming, and muscle atonia.
The sleep cycle repeats approximately every 90 minutes, with REM periods lengthening as the night progresses.
Insomnia: Types, Symptoms, and Consequences
Types of Insomnia
Insomnia can be classified based on duration and underlying causes.
Short-term Insomnia: Lasts less than 3 months; may progress to chronic insomnia.
Chronic Insomnia: Persists for 3 months or longer, with symptoms occurring at least 3 times per week. Often associated with medical, psychiatric, or substance-related issues.
Common Complaints Related to Insomnia
Difficulty falling asleep (increased sleep latency)
Frequent awakenings during the night
Early morning awakening
Inability to return to sleep after awakening
Poor quality or non-restorative sleep

Consequences of Insomnia
Chronic insomnia can lead to significant health and safety risks.
Impaired daytime functioning and fatigue
Mood disturbances: anxiety, irritability, depression
Cognitive impairment: memory problems
Increased risk of accidents (e.g., traffic accidents)
Increased risk of substance abuse, diabetes, heart disease, obesity, and mortality
Medical Conditions and Medications Affecting Sleep
Medical Conditions That May Disrupt Sleep
Several medical and psychiatric conditions can interfere with sleep quality and duration.
Pain disorders, gastrointestinal disorders, respiratory disorders
Diabetes, benign prostatic hyperplasia (BPH), nocturia
Restless legs syndrome, hyperthyroidism, pregnancy, menopause
Bipolar disorder, depression, anxiety, substance abuse
Sleep apnea
Obstructive Sleep Apnea (OSA)
OSA is a common sleep disorder characterized by repeated episodes of upper airway obstruction during sleep.
Results in intermittent hypoxia and sleep fragmentation
Associated with increased cardiovascular risk
Treatment includes weight loss, avoidance of CNS depressants, and use of CPAP (continuous positive airway pressure) devices

Medications That May Disrupt Sleep
Many medications can cause or worsen insomnia.
Stimulants: Caffeine, nicotine, decongestants, β-agonists, amphetamines, cocaine
Other medications: Corticosteroids, antidepressants, antihypertensives, levodopa, MAO-Is, TCAs, opioids
Alcohol: Initially sedating but disrupts sleep architecture and causes rebound insomnia
Substances Affecting Sleep: Alcohol and Caffeine
Effects of Alcohol on Sleep
May help with sleep onset but leads to tolerance, frequent awakenings, and reduced sleep duration
Increases risk of sleep apnea and inhibits caffeine metabolism
Caffeine
Caffeine is a central nervous system stimulant commonly used to counteract drowsiness and fatigue but can cause insomnia and other adverse effects.
Increases heart rate and blood pressure, causes anxiety and tremor
Can complicate pregnancy and lactation, and contribute to kidney stones
Nonpharmacological Management: Sleep Hygiene
Sleep Hygiene Counseling Points
Good sleep hygiene is essential for managing insomnia and improving sleep quality.
Maintain a regular sleep schedule
Ensure a comfortable sleep environment
Engage in relaxing activities before bedtime
Avoid napping and large meals before sleep
Avoid caffeine, alcohol, and nicotine several hours before bedtime
Use the bedroom only for sleep and intimacy
Limit screen time before bed
Pharmacological Management: Antihistamines and Combination Products
Antihistamines for Insomnia
Diphenhydramine: The only FDA-approved antihistamine for sleep
Doxylamine: Used off-label for sleep (25 mg 30 minutes before bedtime)
Other first-generation antihistamines may be used short-term




Combination Products
Many OTC sleep aids combine diphenhydramine with analgesics for patients with pain-related insomnia.
Common combinations: diphenhydramine + acetaminophen, aspirin, ibuprofen, or naproxen
Assess for pain and provide appropriate counseling

Adverse Effects and Precautions
Tolerance, paradoxical CNS stimulation, and anticholinergic toxicity (especially in older adults)
Use should be limited to short-term (maximum 10 days)
Herbal and Dietary Supplements for Sleep
5-HTP (5-Hydroxytryptophan)
Precursor to serotonin; may improve sleep but has significant adverse effects and drug interactions
Associated with eosinophilia myalgia syndrome (EMS); use is not recommended
Melatonin
Endogenous hormone that regulates circadian rhythm
May help with sleep latency, jet lag, and circadian rhythm disorders
Dosing: 0.3–5 mg 30 minutes before bedtime
Adverse effects are rare but include drowsiness, headache, and nausea
Potential drug interactions with anticoagulants, contraceptives, hypoglycemics, immunosuppressants, and antihypertensives

Safety Concerns with Melatonin
Quality and content of OTC melatonin products can be highly variable
Long-term use may be associated with increased risk of heart failure (association, not causation)
OTC melatonin is banned or prescription-only in several countries due to quality concerns
Other Herbal Products
Valerian: Variable efficacy; avoid long-term use due to hepatotoxicity risk
Kava: Not recommended due to risk of liver injury
Other herbs: chamomile, ginseng, lavender, hops, lemon balm, passion flower (limited evidence)
Drowsiness and Fatigue: Caffeine Use and Safety
Caffeine as a Treatment for Drowsiness
CNS stimulant with diuretic effects
Improves alertness, mood, and cognitive performance
Metabolism is inhibited by alcohol and induced by smoking
Dose: 200 mg every 3–4 hours (maximum 600 mg/day)
Adverse effects: anxiety, nausea, increased heart rate and blood pressure, GERD, kidney stones
Caffeine Safety in Special Populations
Pregnancy: <200 mg/day is considered safe; higher intake increases miscarriage risk
Breastfeeding: Caffeine is excreted in breast milk and eliminated slowly in neonates
Children: Unintentional and intentional caffeine exposures are common; caution is advised
When to Refer Patients with Sleep Disorders
Referral Criteria
Children <12 years or adults ≥65 years
Chronic insomnia or significant sleep disturbances
Insomnia secondary to psychiatric or medical conditions
Pregnant or nursing patients
Treatment ineffective after 10 days
Summary Table: Common OTC Sleep Aids and Their Components
Product | Active Ingredient(s) | Indication |
|---|---|---|
Unisom SleepTabs | Doxylamine succinate | Short-term insomnia |
Unisom SleepGels | Diphenhydramine HCl | Short-term insomnia |
ZzzQuil | Diphenhydramine HCl | Short-term insomnia |
Sominex | Diphenhydramine HCl | Short-term insomnia |
Bayer PM | Diphenhydramine + Aspirin | Pain-related insomnia |
Advil PM | Diphenhydramine + Ibuprofen | Pain-related insomnia |
Aleve PM | Diphenhydramine + Naproxen | Pain-related insomnia |
Key Counseling Points
Limit use of OTC sleep aids to short-term management
Practice good sleep hygiene
Be aware of potential adverse effects and drug interactions
Refer patients with complex or persistent sleep disorders to a healthcare provider
