 Back
BackStudy Notes: The Skeletal, Muscular, and Nervous Systems with Endocrine and Sensory Integration
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Chapter 6: The Skeletal System
Functions of the Skeletal System
The skeletal system provides the structural framework for the body and serves several essential physiological roles.
Support: Bones form the framework for the attachment of soft tissues and organs.
Mineral Storage: Bones store calcium and phosphate ions in the bone matrix, essential for metabolic processes.
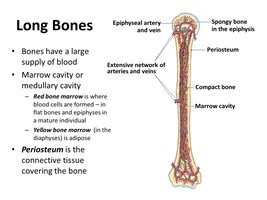
Blood Cell Production: Hematopoiesis occurs in red bone marrow, producing red and white blood cells and platelets.
Protection: Bones such as the skull, thorax, and pelvis protect vital organs from injury.
Movement: Bones act as levers that muscles pull on to generate body motion.
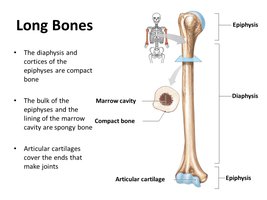
Structure of a Typical Long Bone
Long bones are characterized by distinct anatomical regions and specialized tissues that contribute to their function.
Diaphysis: The central shaft, composed mainly of compact bone, surrounds the medullary (marrow) cavity.
Epiphyses: The expanded ends of the bone, covered with articular cartilage, contain spongy bone.
Periosteum: The outer surface membrane, providing nourishment and attachment for tendons and ligaments.
Endosteum: The inner membrane lining the marrow cavity and spongy bone.
Bone Cells and Calcium Homeostasis
Bone tissue contains three primary cell types, each with distinct functions in bone maintenance and remodeling. Calcium homeostasis is tightly regulated by hormonal control.
Osteocytes: Mature bone cells residing in lacunae; maintain bone matrix.
Osteoblasts: Bone-forming cells that synthesize and secrete bone matrix; become osteocytes when surrounded by matrix.
Osteoclasts: Large, multinucleated cells that resorb bone matrix, releasing minerals into the blood.
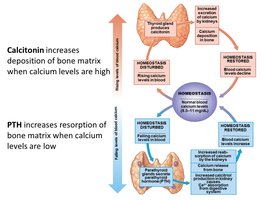
Calcium Homeostasis:
Calcitonin: Lowers blood calcium by promoting deposition in bone.
Parathyroid Hormone (PTH): Raises blood calcium by stimulating bone resorption and increasing intestinal absorption.
Bone Growth and Development
Bones grow and develop through two primary processes: intramembranous and endochondral ossification.
Intramembranous Ossification: Formation of flat bones from fibrous connective tissue (e.g., skull, clavicle).
Endochondral Ossification: Most bones form from hyaline cartilage templates; primary ossification center in diaphysis, secondary centers in epiphyses.
Epiphyseal Plate: Cartilage between diaphysis and epiphysis allows for lengthwise growth until ossification completes at puberty, forming the epiphyseal line.
Appositional Growth: Increase in bone diameter by adding new layers under the periosteum.
Clinical Disorders of Bone Growth
Abnormal bone growth and development can lead to various clinical disorders:
Osteoporosis: Decreased bone density and increased fracture risk.
Gigantism: Excess growth hormone before puberty; abnormal height.
Acromegaly: Excess growth hormone after puberty; thickened bones and soft tissues.
Pituitary Growth Failure: Reduced cartilage activity; short stature.
Marfan’s Syndrome: Excessive cartilage growth; tall, slender limbs, cardiovascular issues.
Achondroplasia: Early fusion of epiphyseal plates; short limbs, normal trunk.
Fibrodysplasia Ossificans Progressiva: Abnormal ossification of connective tissues.
Chapter 7: The Muscular System
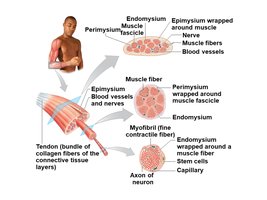
Organization of Skeletal Muscle Tissue
Skeletal muscles are organized into bundles surrounded by connective tissue layers, which provide structure and transmit force.
Endomysium: Surrounds individual muscle fibers.
Perimysium: Bundles fibers into fascicles.
Epimysium: Encloses the entire muscle organ.
Tendon: Cord-like structure attaching muscle to bone.
Aponeurosis: Broad, flat connective tissue sheet.
Types of Muscle Tissue
Muscle tissue is classified into three types based on structure, location, and function.
Skeletal Muscle: Long, cylindrical, striated, multinucleate fibers; voluntary control; attached to skeleton.
Cardiac Muscle: Short, branched, striated cells with one or two nuclei; involuntary; found in the heart; intercalated discs for communication.
Smooth Muscle: Short, spindle-shaped, unstriated cells with one nucleus; involuntary; found in walls of hollow organs.
Structure of a Skeletal Muscle Fiber and Neuromuscular Junction
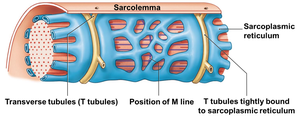
Skeletal muscle fibers contain specialized structures for contraction and communication with nerves.
Sarcolemma: Plasma membrane of the muscle fiber.
Sarcoplasm: Cytoplasm of the muscle fiber.
Sarcoplasmic Reticulum (SR): Stores calcium ions, essential for contraction.
Myofibrils: Contractile organelles made of repeating sarcomeres.
Transverse Tubules (T-tubules): Conduct action potentials from the sarcolemma to the SR.
Thin Filament: Composed of actin, tropomyosin, and troponin.
Thick Filament: Composed of myosin; heads form cross-bridges with actin.
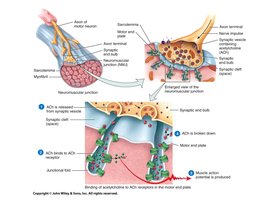
Neuromuscular Junction: Synapse between a motor neuron and a muscle fiber; site of neurotransmitter (acetylcholine) release.
Excitation-Contraction Coupling
Muscle contraction is initiated by nerve impulses and involves a series of steps linking excitation to contraction.
Neurons release acetylcholine (ACh) at the neuromuscular junction.
ACh binds to receptors on the sarcolemma, opening sodium channels and generating an action potential.
Action potential travels down T-tubules, triggering calcium release from the SR.
Calcium binds to troponin, shifting tropomyosin and exposing actin binding sites.
Myosin heads bind to actin, forming cross-bridges and pulling thin filaments toward the M line (sliding filament theory).
ATP is required for myosin head detachment and resetting.
Relaxation occurs via gravity, opposing muscles, or elastic recoil.
Motor Unit Recruitment and Tension Generation
The force generated by a muscle depends on the number of motor units activated.
Motor Unit: One motor neuron and all the muscle fibers it controls.
Recruitment: Activation of additional motor units increases muscle tension.
Muscle Tone: Resting tension maintained by some motor units even when the muscle is not contracting.
Muscle Hypertrophy, Atrophy, and Rigor Mortis
Hypertrophy: Increase in muscle size due to increased fiber size from repeated stimulation.
Atrophy: Decrease in muscle size due to lack of use or nerve supply.
Rigor Mortis: Stiffening of muscles after death due to lack of ATP for relaxation.
Chapter 8: The Nervous System
Functional and Structural Divisions
The nervous system is divided into central and peripheral components, each with specialized functions.
Central Nervous System (CNS): Brain and spinal cord; integration and processing of information.
Peripheral Nervous System (PNS): Cranial and spinal nerves; sensory (afferent) and motor (efferent) divisions.
Somatic Nervous System (SNS): Voluntary control of skeletal muscles.
Autonomic Nervous System (ANS): Involuntary control of smooth/cardiac muscle, glands, adipose tissue; includes sympathetic (fight or flight) and parasympathetic (rest and digest) divisions.
Neurons and Neuroglia
Neurons are specialized for impulse transmission, while neuroglia support and protect neurons.
Neuron Structure: Cell body, dendrites (receive signals), axon (transmits signals), axon hillock, axon terminal (neurotransmitter release).
Types of Neurons: Unipolar, bipolar, multipolar; classified by structure and location.
Synapse: Junction between two neurons or a neuron and effector; presynaptic and postsynaptic components.
Neuroglia: Support cells; types include astrocytes, microglia, ependymal cells, oligodendrocytes (CNS), satellite cells, and Schwann cells (PNS).
Myelin: Lipid-rich sheath that increases conduction speed; white matter (myelinated), gray matter (unmyelinated/cell bodies).
Functional Anatomy of the Brain and Spinal Cord
Cerebrum: Conscious thought, memory, sensory processing, voluntary movement.
Cerebellum: Coordination, balance, motor modulation.
Diencephalon: Thalamus (sensory relay), hypothalamus (autonomic/hormonal control).
Brain Stem: Midbrain (reflexes), pons (relay), medulla oblongata (vital functions).
Spinal Cord: Enlargements for limb control, conus medullaris, cauda equina.
Reflex Arcs
Reflexes are rapid, involuntary responses to stimuli, preserving homeostasis.
Components: Receptor, sensory neuron, integration center, motor neuron, effector.
Monosynaptic Reflex: Simple, fast (e.g., stretch reflex).
Polysynaptic Reflex: Complex, slower (e.g., withdrawal reflex).
Autonomic Nervous System: Sympathetic vs. Parasympathetic
Sympathetic: Thoracolumbar origin, short preganglionic/long postganglionic fibers, widespread effects, "fight or flight" (increased heart rate, metabolic rate, etc.).
Parasympathetic: Craniosacral origin, long preganglionic/short postganglionic fibers, localized effects, "rest and digest" (decreased heart rate, increased digestion, etc.).
Chapter 9: The General and Special Senses
General and Special Senses
Sensory receptors detect changes in the environment and relay information to the nervous system.
General Senses: Temperature, pain, touch, pressure, vibration, proprioception.
Receptor Types: Nociceptors (pain), thermoreceptors (temperature), mechanoreceptors (stretch, pressure, vibration), chemoreceptors (chemical concentrations).
Special Senses: Olfaction (smell), gustation (taste), vision, hearing, equilibrium; located in specialized organs.
Functional Anatomy of Special Sense Organs
Olfaction: Receptor cells in nasal cavity; signals relayed via olfactory nerve to cortex.
Gustation: Taste buds on tongue; signals via cranial nerves to gustatory cortex.
Vision: Eye structures include cornea, lens, retina (rods/cones), optic nerve; image processing and depth perception.
Hearing/Equilibrium: Outer, middle, inner ear structures; cochlea (hearing), vestibule/semicircular canals (balance).
Chapter 10: The Endocrine System
Hormones and Their Functions
The endocrine system regulates physiological processes via hormones secreted by glands.
Pituitary Gland: Releases hormones controlling other glands (e.g., TSH, ACTH, GH, PRL, FSH, LH, ADH, OXT).
Thyroid Gland: T3/T4 increase metabolism; calcitonin lowers blood calcium.
Parathyroid Glands: PTH raises blood calcium.
Pancreas: Insulin lowers, glucagon raises blood glucose.
Pineal Gland: Melatonin regulates circadian rhythms.
Gonads: Produce sex hormones and gametes.
Adrenal Glands: Cortex produces steroids; medulla produces epinephrine/norepinephrine.
Mechanisms of Hormone Action
Nonsteroid Hormones: Bind to cell surface receptors, activate second messengers (e.g., cAMP); rapid, short-lived effects.
Steroid Hormones: Cross membranes, bind intracellular receptors, alter gene expression; slower, longer-lasting effects.
Endocrine Disorders
Hypersecretion: Excess hormone production.
Hyposecretion: Insufficient hormone production; can be primary (gland problem) or secondary (stimulating hormone problem).
Nervous vs. Endocrine System Control
Both: Use chemical messengers, maintain homeostasis, often via negative feedback.
Nervous System: Fast, short-lived, point-to-point connectivity.
Endocrine System: Slower, longer-lasting, widespread effects via bloodstream.
