 Back
BackThe Cardiovascular System: The Heart – Structure, Function, and Clinical Relevance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Cardiovascular System: The Heart
Introduction
The heart is a muscular organ essential for pumping blood throughout the body, supplying tissues with oxygen and nutrients, and removing waste products. Understanding its anatomy, physiology, and clinical significance is crucial for students of human anatomy and physiology.
Clinical Case: Chest Pain
Recognizing Cardiac Emergencies
Symptoms of Heart Attack: Chest pain (often central and radiating to the left arm), diaphoresis (sweating), shortness of breath, and palpitations are concerning for myocardial infarction (heart attack).
Risk Factors: Smoking and hypertension are major risk factors for coronary artery disease and heart attacks.
Normal Values: Normal blood pressure is ≤120/80 mmHg; normal heart rate is 60–100 bpm.
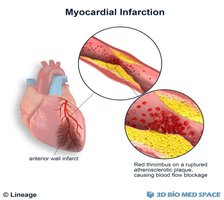
Thrombus: A thrombus is a blood clot that forms in a vessel and can obstruct blood flow, leading to tissue ischemia or infarction.

Overview and Learning Goals
Describe the two main circulation routes (pulmonary and systemic circuits).
Identify the heart’s anatomical location and coverings.
Recognize major internal and external heart structures.
Trace the flow of blood through the heart.
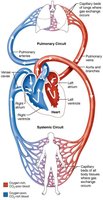
Pulmonary and Systemic Circuits
Dual Circulation Pathways
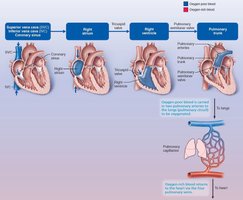
Pulmonary Circuit: Right side of the heart pumps oxygen-poor blood to the lungs for gas exchange (removal of CO2, uptake of O2).
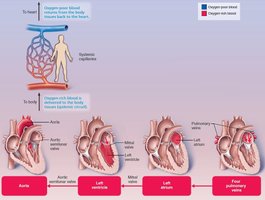
Systemic Circuit: Left side of the heart pumps oxygen-rich blood to the body tissues.
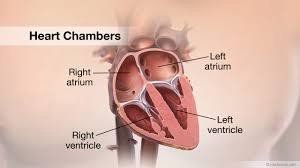
Heart Chambers and Major Vessels
Internal and External Anatomy
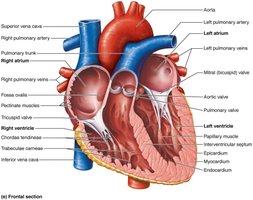
Chambers: The heart has four chambers: two atria (receiving chambers) and two ventricles (pumping chambers).
Right Atrium: Receives deoxygenated blood from the body via the superior and inferior vena cava and the coronary sinus.
Left Atrium: Receives oxygenated blood from the lungs via four pulmonary veins.
Right Ventricle: Pumps blood to the lungs via the pulmonary trunk.
Left Ventricle: Pumps blood to the systemic circulation via the aorta.
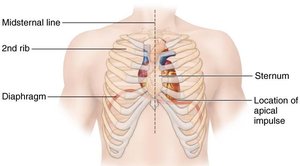
Size, Location, and Orientation of the Heart
Anatomical Position
The heart is about the size of a fist and weighs less than 1 pound.
Located in the mediastinum, between the 2nd and 5th intercostal spaces, posterior to the sternum, and anterior to the spine.
The apex points toward the left hip; the base leans toward the right shoulder.
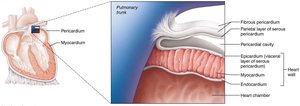
Coverings and Layers of the Heart
Pericardium and Heart Wall
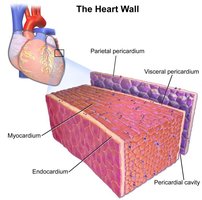
Pericardium: Double-walled sac with a superficial fibrous layer (protection, anchoring, prevents overfilling) and a deep serous layer (parietal and visceral/epicardium layers).
Pericardial Cavity: Fluid-filled space between layers reduces friction.
Heart Wall Layers: Epicardium (outer), myocardium (muscular middle), endocardium (inner lining).

Clinical Significance: Pericarditis and Cardiac Tamponade
Pericarditis: Inflammation of the pericardium, causing friction rub and pain.
Cardiac Tamponade: Accumulation of fluid in the pericardial cavity compresses the heart, requiring emergency drainage (pericardiocentesis).
Heart Valves
Types and Functions
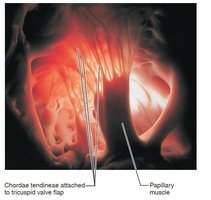
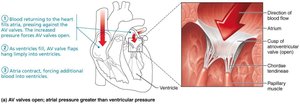
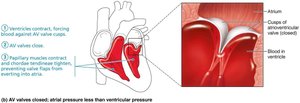
Atrioventricular (AV) Valves: Tricuspid (right) and mitral/bicuspid (left) valves prevent backflow into atria during ventricular contraction. Chordae tendineae anchor valve flaps to papillary muscles.
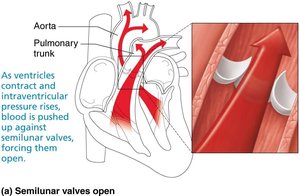
Semilunar (SL) Valves: Pulmonary (right ventricle to pulmonary trunk) and aortic (left ventricle to aorta) valves prevent backflow from arteries into ventricles.

Clinical Significance: Valve Disorders
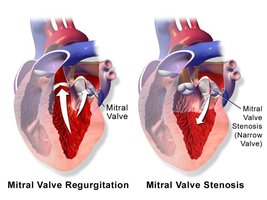
Incompetent Valve (Regurgitation): Valve fails to close completely, causing blood to flow backward.
Valvular Stenosis: Valve flaps become stiff, narrowing the opening and increasing cardiac workload.
Defective valves may be replaced with mechanical or biological prostheses.
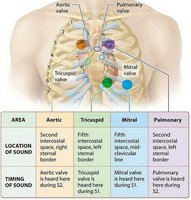
Heart Sounds and Murmurs
Normal and Abnormal Heart Sounds
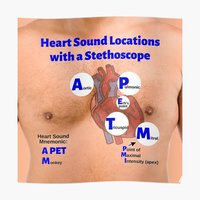
Normal Sounds: "Lub-dub" sounds correspond to AV and SL valve closure.
Murmurs: Abnormal sounds due to turbulent blood flow, often from valve defects.
Pathway of Blood Through the Heart
Right Side (Pulmonary Circuit)
Blood enters right atrium from SVC, IVC, and coronary sinus → tricuspid valve → right ventricle → pulmonary semilunar valve → pulmonary trunk → pulmonary arteries → lungs.
Left Side (Systemic Circuit)
Oxygenated blood returns via four pulmonary veins → left atrium → mitral valve → left ventricle → aortic semilunar valve → aorta → systemic circulation.
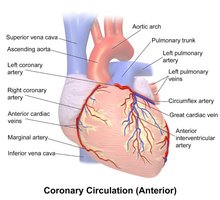
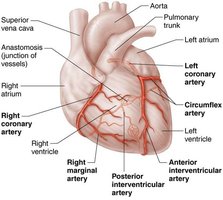
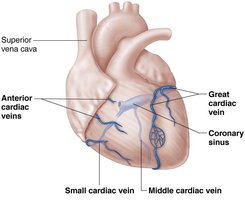
Coronary Circulation
Supplying the Heart Muscle
Coronary Arteries: Left (anterior interventricular and circumflex branches) and right (right marginal and posterior interventricular branches) supply the myocardium.
Coronary Veins: Great, middle, and small cardiac veins drain into the coronary sinus, which empties into the right atrium.
Clinical Significance: Angina and Myocardial Infarction
Angina Pectoris: Chest pain from transient myocardial ischemia.
Myocardial Infarction (Heart Attack): Prolonged coronary blockage leads to cell death and scar formation.
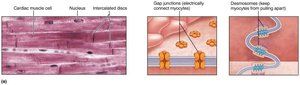
Microscopic Anatomy of Cardiac Muscle
Structure and Function
Cardiac muscle cells are striated, branched, and interconnected by intercalated discs containing gap junctions and desmosomes.
Gap junctions allow ions to pass, enabling the heart to contract as a functional syncytium.
Cardiac muscle relies almost exclusively on aerobic respiration and contains abundant mitochondria.
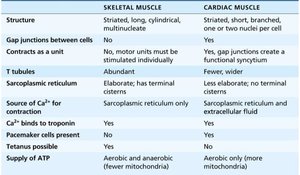
Feature | Skeletal Muscle | Cardiac Muscle |
|---|---|---|
Structure | Striated, long, cylindrical, multinucleate | Striated, short, branched, 1–2 nuclei/cell |
Gap Junctions | No | Yes |
Pacemaker Cells | No | Yes |
ATP Supply | Aerobic and anaerobic | Aerobic only (more mitochondria) |
Conduction System of the Heart
Intrinsic Cardiac Conduction
The heart generates its own electrical impulses via pacemaker cells.
Sequence: Sinoatrial (SA) node → Atrioventricular (AV) node → Bundle of His → Right and left bundle branches → Purkinje fibers.
SA node sets the pace (sinus rhythm, 60–100 bpm); AV node delays impulse to allow atrial contraction.
Clinical Significance: Arrhythmias and Heart Block
Arrhythmias are abnormal rhythms; fibrillation is rapid, uncoordinated contraction.
Heart block occurs when AV node conduction is impaired; may require a pacemaker.
Electrocardiography (ECG/EKG)
Recording Heart’s Electrical Activity
P wave: Atrial depolarization
QRS complex: Ventricular depolarization (and atrial repolarization)
T wave: Ventricular repolarization
Clinical Significance
ECG changes can indicate heart disease, ischemia, or conduction problems (e.g., ST elevation in myocardial infarction).
Mechanical Events of the Heart (Cardiac Cycle)
Phases of the Cardiac Cycle
Systole: Contraction phase
Diastole: Relaxation phase
One cardiac cycle lasts about 0.8 seconds at 75 bpm.
Ventricular Filling
During diastole, ventricles fill passively (80%) and then actively (20%) during atrial contraction.
End Diastolic Volume (EDV): Volume of blood in ventricles at end of diastole.
Isovolumetric Contraction
Ventricles contract with all valves closed; pressure rises until SL valves open.
Ventricular Ejection
SL valves open; blood is ejected into aorta and pulmonary trunk.
Isovolumetric Relaxation
Ventricles relax; SL valves close; End Systolic Volume (ESV): blood remaining after contraction.
Cardiac Output (CO)
Definition and Calculation
CO is the amount of blood pumped by each ventricle per minute.
Formula:
At rest:
Regulation of Stroke Volume (SV)
Formula:
Factors: Preload (stretch), contractility (force), afterload (arterial pressure).
Regulation of Heart Rate
Autonomic and Hormonal Control
Sympathetic Stimulation: Increases HR and contractility (norepinephrine, epinephrine).
Parasympathetic Stimulation: Decreases HR (acetylcholine via vagus nerve).
Hormones: Epinephrine and thyroxine increase HR; ion imbalances (Ca2+, K+) can be dangerous.
Clinical Significance: Heart Rate Abnormalities
Tachycardia: HR > 100 bpm; may lead to fibrillation.
Bradycardia: HR < 60 bpm; may be normal in athletes but problematic if symptomatic.
Cardiac Output Abnormalities
Congestive Heart Failure (CHF)
CO is insufficient to meet tissue needs; caused by coronary artery disease, hypertension, or myocardial infarction.
Left-sided failure: pulmonary congestion; right-sided failure: peripheral edema.
Developmental Aspects and Congenital Heart Defects
Fetal structures (foramen ovale, ductus arteriosus) bypass pulmonary circulation; close after birth.
Congenital defects include septal defects and valve/vessel narrowing (e.g., Tetralogy of Fallot).
