 Back
BackThe Endocrine System: Structure, Function, and Regulation
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Endocrine System
Overview of the Endocrine System
The endocrine system works in concert with the nervous system to coordinate and integrate the activity of body cells. It influences metabolic activities through hormones transported in the blood. Endocrine responses occur more slowly but last longer than those of the nervous system.
Hormones: Long-distance chemical signals that travel in the blood or lymph.
Autocrines: Chemicals that exert effects on the same cells that secrete them.
Paracrines: Locally acting chemicals that affect cells other than those that secrete them.
Only hormones are considered part of the endocrine system.
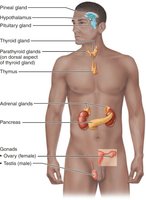
Location of Selected Endocrine Organs
Major endocrine glands include the pineal gland, hypothalamus, pituitary gland, thyroid gland, parathyroid glands, thymus, adrenal glands, pancreas, and gonads (ovaries and testes).
Chemical Messengers and Hormone Classes
Chemistry of Hormones
Hormones are classified into two main groups based on their chemical structure:
Amino acid-based hormones: Includes amines, thyroxine, peptides, and proteins.
Steroid hormones: Synthesized from cholesterol; includes gonadal and adrenocortical hormones.
Mechanisms of Hormone Action
Water-Soluble vs. Lipid-Soluble Hormones
Hormones act through two primary mechanisms depending on their solubility:
Water-soluble hormones: (All amino acid–based hormones except thyroid hormone) act on plasma membrane receptors and are coupled by G proteins to intracellular second messengers.
Lipid-soluble hormones: (Steroid and thyroid hormones) act on intracellular receptors that directly activate genes.
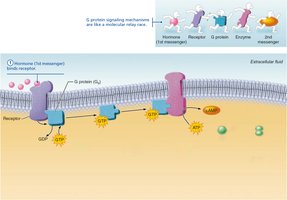
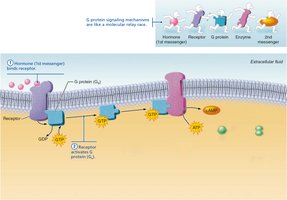
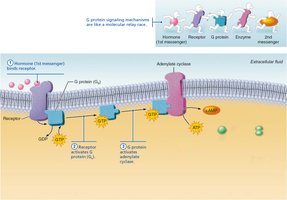
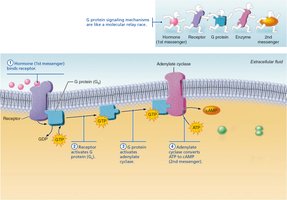
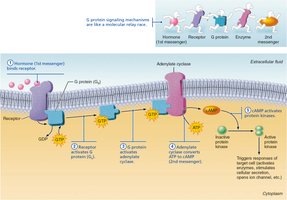
Cyclic AMP (cAMP) Signaling Mechanism
The cAMP pathway is a common mechanism for water-soluble hormones. It involves a relay of molecular events leading to cellular responses.
Hormone binds to receptor.
Receptor activates G protein.
G protein activates adenylate cyclase.
Adenylate cyclase converts ATP to cAMP (second messenger).
cAMP activates protein kinases, which trigger cellular responses.
Intracellular Receptors and Direct Gene Activation
Lipid-soluble hormones diffuse through the plasma membrane and bind to intracellular receptors, which then directly activate genes by stimulating transcription.
Steroid hormone enters cell and binds to receptor.
Receptor-hormone complex enters nucleus.
Complex binds to specific DNA regions.
Binding initiates transcription of the gene to mRNA.
mRNA directs protein synthesis.





Target Cell Specificity and Activation
Target Cell Specificity
Target cells must have specific receptors for a hormone to bind and exert its effects. For example, ACTH receptors are only found on certain cells of the adrenal cortex, while thyroxin receptors are found on nearly all cells of the body.
Factors Affecting Target Cell Activation
Blood levels of the hormone
Relative number of receptors on or in the target cell
Affinity of binding between receptor and hormone
Hormones can influence the number of their receptors:
Up-regulation: Target cells form more receptors in response to the hormone.
Down-regulation: Target cells lose receptors in response to the hormone.
Hormones in the Blood
Transport and Removal
Hormones circulate in the blood either free or bound to plasma proteins. Steroids and thyroid hormone are attached to plasma proteins, while others circulate without carriers. The concentration of a circulating hormone reflects its rate of release and speed of inactivation/removal from the body.
Hormones are removed by degrading enzymes, kidneys, and liver.
Half-life: The time required for a hormone’s blood level to decrease by half.
Hormone Interactions and Control
Interaction of Hormones at Target Cells
Permissiveness: One hormone cannot exert its effects without another hormone being present.
Synergism: More than one hormone produces the same effects on a target cell.
Antagonism: One or more hormones opposes the action of another hormone.
Control of Hormone Release
Blood levels of hormones are controlled by negative feedback systems and vary only within a narrow desirable range. Hormones are synthesized and released in response to humoral, neural, and hormonal stimuli.
Humoral Stimuli
Changing blood levels of ions and nutrients directly stimulate secretion of hormones. For example, low Ca2+ in blood stimulates secretion of parathyroid hormone (PTH).
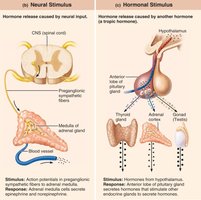
Neural Stimuli
Nerve fibers stimulate hormone release, such as the stimulation of the adrenal medulla by the sympathetic nervous system.
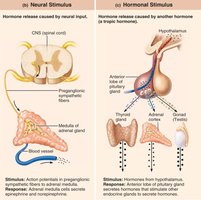
Hormonal Stimuli
Hormones stimulate other endocrine organs to release their hormones, such as the hypothalamic hormones stimulating the anterior pituitary.
Nervous System Modulation
The nervous system can modify the stimulation of endocrine glands and their negative feedback mechanisms. For example, under severe stress, the hypothalamus and sympathetic nervous system are activated, causing body glucose levels to rise.
Anterior Pituitary Hormones
Growth Hormone (GH)
Produced by somatotrophs, GH stimulates most cells, especially bone and skeletal muscle. It promotes protein synthesis and encourages the use of fats for fuel. Most effects are mediated indirectly by insulin-like growth factors (IGFs).
Homeostatic Imbalances of Growth Hormone
Hypersecretion: In children, results in gigantism; in adults, results in acromegaly.
Hyposecretion: In children, results in pituitary dwarfism.

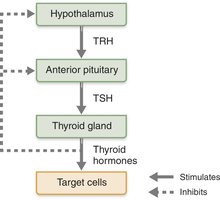
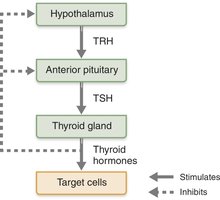
Thyroid-Stimulating Hormone (TSH)
Produced by thyrotrophs of the anterior pituitary, TSH stimulates the normal development and secretory activity of the thyroid gland. Regulation of TSH release is stimulated by thyrotropin-releasing hormone (TRH) and inhibited by rising blood levels of thyroid hormones.
Adrenocorticotropic Hormone (ACTH)
Secreted by corticotrophs of the anterior pituitary, ACTH stimulates the adrenal cortex to release corticosteroids. Its release is triggered by hypothalamic corticotropin-releasing hormone (CRH) in a daily rhythm and can be altered by internal and external factors such as fever, hypoglycemia, and stressors.
Gonadotropins (FSH and LH)
Follicle-stimulating hormone (FSH) and luteinizing hormone (LH) are secreted by gonadotrophs. FSH stimulates gamete production, while LH promotes production of gonadal hormones. Their release is triggered by gonadotropin-releasing hormone (GnRH) during and after puberty and suppressed by gonadal hormones.
Prolactin (PRL)
Secreted by lactotrophs, PRL stimulates milk production. Its release is primarily controlled by prolactin-inhibiting hormone (PIH, dopamine). Blood levels rise toward the end of pregnancy, and suckling stimulates PRH release and promotes continued milk production.
Posterior Pituitary Hormones
Oxytocin
Oxytocin stimulates uterine contractions during childbirth by mobilizing Ca2+ through a PIP2-Ca2+ second-messenger system. It also triggers milk ejection in women producing milk and plays a role in sexual arousal and orgasm in both sexes.
Antidiuretic Hormone (ADH)
ADH is released in response to high solute concentration in the blood, inhibiting urine formation. Alcohol inhibits ADH release, causing copious urine output. Homeostatic imbalances include diabetes insipidus (ADH deficiency) and syndrome of inappropriate ADH secretion (SIADH).
Thyroid Hormone
Thyroid Hormone (TH)
TH consists of two related compounds: T4 (thyroxine) and T3 (triiodothyronine). It is the major metabolic hormone, increasing metabolic rate and heat production, and plays roles in blood pressure maintenance, tissue growth regulation, development of skeletal and nervous systems, and reproductive capabilities.
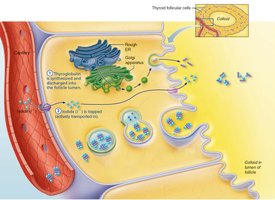
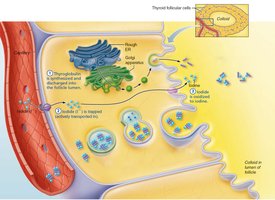
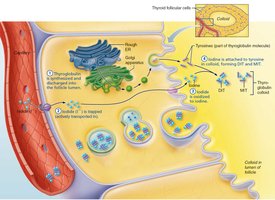
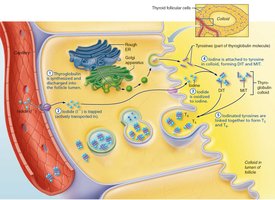
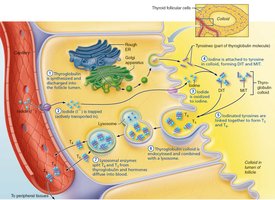
Synthesis of Thyroid Hormone
The synthesis of TH involves several steps, including the production and discharge of thyroglobulin, trapping and modification of iodide, and coupling of iodinated tyrosines to form T3 and T4.

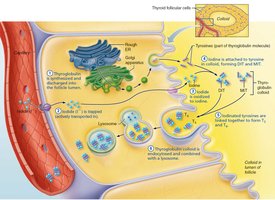
Transport and Regulation of TH
T4 and T3 are transported by thyroxine-binding globulins (TBGs). Both bind to target receptors, but T3 is ten times more active than T4. Peripheral tissues convert T4 to T3. Negative feedback regulation of TH release occurs as rising TH levels inhibit TSH release.
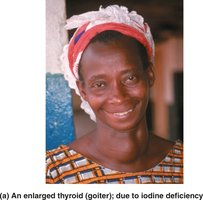
Homeostatic Imbalances of TH
Hyposecretion: In adults, results in myxedema and can lead to endemic goiter if due to lack of iodine. In infants, leads to cretinism.
Hypersecretion: Results in hyperthyroidism, most commonly Graves’ Disease.

Calcitonin
Produced by parafollicular (C) cells, calcitonin is an antagonist to parathyroid hormone (PTH). It inhibits osteoclast activity and release of Ca2+ from bone matrix, but has a limited role in humans.
Parathyroid Hormone
Functions of Parathyroid Hormone (PTH)
Stimulates osteoclasts to digest bone matrix.
Enhances reabsorption of Ca2+ and secretion of phosphate by the kidneys.
Promotes activation of vitamin D, increasing absorption of Ca2+ by intestinal mucosa.
Negative feedback control: rising Ca2+ in the blood inhibits PTH release.

Homeostatic Imbalances of PTH
Hyperparathyroidism: Bones soften and deform; elevated Ca2+ depresses the nervous system and contributes to kidney stones.
Hypoparathyroidism: Results in tetany, respiratory paralysis, and death.
Adrenal Hormones
Mineralocorticoids
Mineralocorticoids regulate electrolytes in extracellular fluid. Aldosterone is the most potent, stimulating Na+ reabsorption and water retention by the kidneys.
Mechanisms of Aldosterone Secretion
Renin-angiotensin mechanism: Decreased blood pressure stimulates kidneys to release renin, triggering formation of angiotensin II, which stimulates aldosterone release.
Plasma concentration of K+: Increased K+ directly influences aldosterone release.
ACTH: Causes small increases of aldosterone during stress.
Atrial natriuretic peptide (ANP): Blocks renin and aldosterone secretion to decrease blood pressure.

Homeostatic Imbalances of Aldosterone
Aldosteronism: Hypersecretion due to adrenal tumors; causes hypertension, edema, and abnormal function of neurons and muscle.
Glucocorticoids (Cortisol)
Glucocorticoids keep blood sugar levels relatively constant and maintain blood pressure by increasing the action of vasoconstrictors. Cortisol is the most significant glucocorticoid, released in response to ACTH, eating/activity patterns, and stress. Its prime metabolic effect is gluconeogenesis—formation of glucose from fats and proteins.
Promotes rises in blood glucose, fatty acids, and amino acids.
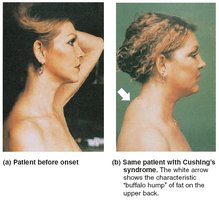
Homeostatic Imbalances of Glucocorticoids
Hypersecretion: Cushing’s syndrome; depresses cartilage and bone formation, inhibits inflammation, depresses immune system, and promotes changes in cardiovascular, neural, and gastrointestinal function.
Hyposecretion: Addison’s disease; involves deficits in mineralocorticoids, decrease in glucose and Na+ levels, weight loss, severe dehydration, and hypotension.
Gonadocorticoids (Sex Hormones)
Most are androgens (male sex hormones) converted to testosterone or estrogens. They contribute to puberty onset, secondary sex characteristics, and sex drive.
Adrenal Medulla
Chromaffin cells secrete epinephrine (80%) and norepinephrine (20%), causing blood glucose levels to rise, blood vessels to constrict, heart rate to increase, and blood to be diverted to the brain, heart, and skeletal muscle.
Stress and the Adrenal Gland
The adrenal gland responds to both short-term and long-term stress, affecting cardiovascular, metabolic, and renal functions.


Pineal Secretions
Pineal Gland
The pineal gland secretes melatonin, which may affect timing of sexual maturation, day/night cycles, and physiological processes with rhythmic variations.
Pancreatic Secretions
Glucagon
Glucagon's major target is the liver, where it promotes glycogenolysis (breakdown of glycogen to glucose), gluconeogenesis (synthesis of glucose from lactic acid and noncarbohydrates), and release of glucose to the blood.
Insulin
Insulin lowers blood glucose levels, enhances membrane transport of glucose into fat and muscle cells, participates in neuronal development, and inhibits glycogenolysis and gluconeogenesis. It activates a tyrosine kinase enzyme receptor, leading to increased glucose uptake and enzymatic activities.
Catalyzes oxidation of glucose for ATP production.
Polymerizes glucose to form glycogen.
Converts glucose to fat (especially in adipose tissue).

Homeostatic Imbalances of Insulin
Diabetes mellitus (DM): Due to hyposecretion or hypoactivity of insulin. Cardinal signs include polyuria, polydipsia, and polyphagia.
Hyperinsulinism: Excessive insulin secretion; results in hypoglycemia, disorientation, unconsciousness.
Types of Diabetes Mellitus
Type 1 (insulin dependent): Autoimmune disease where the body destroys beta cells.
Type 2 (non-insulin dependent): Most common; usually develops in middle age. Beta cells produce insulin, but body cells no longer recognize it effectively (down-regulation).
Sex Hormones
Ovaries and Placenta
Ovaries produce estrogens and progesterone, responsible for maturation of female reproductive organs, appearance of female secondary sexual characteristics, breast development, and cyclic changes in the uterine mucosa. The placenta secretes estrogens, progesterone, and human chorionic gonadotropin (hCG).
Testes
Testes produce testosterone, which initiates maturation of male reproductive organs, causes appearance of male secondary sexual characteristics and sex drive, is necessary for normal sperm production, and maintains functionality of reproductive organs.
Developmental Aspects
Hormonal Changes with Age
Ovaries become unresponsive to gonadotropins with age, leading to estrogen deficiency.
Testosterone diminishes with age, but effects are not usually seen until very old age.
GH levels decline with age, accounting for muscle atrophy.
TH declines with age, contributing to lower basal metabolic rates.
PTH levels remain fairly constant, but lack of estrogen in older women increases vulnerability to bone-demineralizing effects of PTH.
