 Back
BackThe Female Reproductive System: Structure, Function, and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Female Reproductive System: Overview
Main Functions
The female reproductive system is responsible for producing gametes (eggs), providing nutrition and space for fetal development, giving birth, and nourishing the infant. It consists of primary and secondary sex organs, each with specialized roles in reproduction and development.
Primary sex organ: Ovary – produces eggs and hormones.
Secondary sex organs: Uterine tubes, uterus, vagina, and external genitalia.
Ovaries
Structure and Function
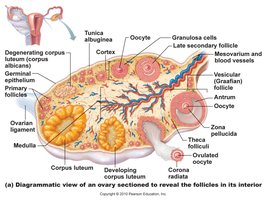
The ovaries are almond-shaped organs (3 cm x 1.5 cm) that produce eggs (oocytes) and secrete hormones such as estrogen and progesterone. Each egg develops within a fluid-filled follicle and is released during ovulation.
Cortex: Produces gametes (oocytes).
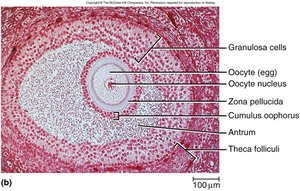
Medulla: Contains blood vessels and nerves.
Follicle: Structure where the egg matures; surrounded by granulosa cells.
Uterine (Fallopian) Tubes
Anatomy and Function
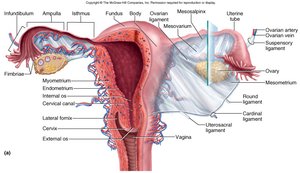
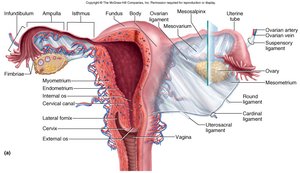
The uterine tubes are muscular tubes (~10 cm long) lined with ciliated cells. They transport the ovulated egg from the ovary to the uterus. The distal end flares into the infundibulum, which is fringed with fimbriae that help capture the egg.
Cilia: Propel the egg toward the uterus.
Infundibulum and fimbriae: Capture the released oocyte.
Uterus
Structure and Layers
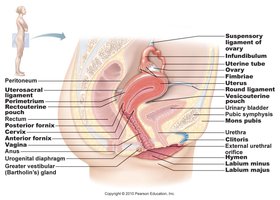
The uterus is a thick-walled, pear-shaped muscular chamber that opens into the vagina and tilts forward over the bladder. It is the site of implantation and fetal development.
Fundus: Upper rounded region.
Body: Main part of the uterus.
Cervix: Lower, narrow portion opening into the vagina.
Histology of the Uterine Wall
Perimetrium: External serous layer.
Myometrium: Thick, middle smooth muscle layer; responsible for contractions during labor.
Endometrium: Inner mucosal layer; has a functional layer (shed during menstruation) and a basal layer (regenerates the functional layer).
Vagina and External Genitalia
Vagina
The vagina is an 8-10 cm muscular tube that allows for the discharge of menstrual fluid, receipt of the penis and semen, and birth of the baby. It is lined with rugae and has an acidic pH due to bacterial fermentation, which provides protection against pathogens.
No glands: Lubrication is provided by cervical mucus.
Rugae: Folds that allow for expansion.
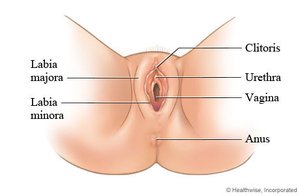
Vulva (Pudendum)
The vulva includes the external genital structures:
Mons pubis: Fatty mound over the pubic symphysis.
Labia majora: Thick, outer folds of skin.
Labia minora: Thin, inner folds; form the vestibule and prepuce over the clitoris.
Clitoris: Erectile, sensory organ.
Vestibular glands: Provide lubrication.
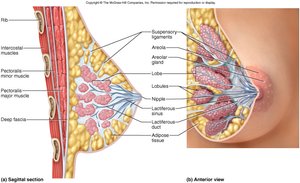
Breasts and Mammary Glands
Structure and Function
The breasts contain mammary glands, which are specialized for milk production. Each gland has 15-20 lobes, each with a lactiferous duct leading to the nipple. The areola surrounds the nipple and darkens during pregnancy.
Lactiferous ducts: Transport milk to the nipple.
Adipose tissue: Provides shape and size to the breast.
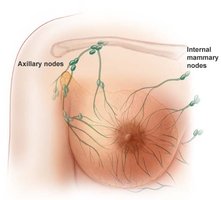
Lymphatic vessels: Drain into axillary and internal mammary nodes.
Breast Cancer
Overview and Risk Factors
Breast cancer is a common malignancy in women, often originating from the cells of the mammary ducts. It may metastasize via lymphatic vessels. Risk factors include early menarche, late menopause, aging, exposure to radiation, certain chemicals, alcohol, smoking, and high fat intake. Most cases are nonhereditary, but mutations in BRCA1 and BRCA2 genes increase risk.
Symptoms: Palpable lump, skin puckering, changes in skin texture, nipple discharge.
Screening: Mammograms, ultrasound, MRI (for high-risk individuals).
Treatment: Lumpectomy, mastectomy, radiation, chemotherapy, hormone therapy (e.g., tamoxifen).
Puberty and Hormonal Regulation
Onset and Hormonal Changes
Puberty in females typically begins between ages 9-10 and is triggered by increased secretion of gonadotropin-releasing hormone (GnRH), which stimulates the anterior pituitary to release follicle-stimulating hormone (FSH) and luteinizing hormone (LH). These hormones promote the development of ovarian follicles and the secretion of estrogen and progesterone.
Thelarche: Breast development.
Pubarche: Growth of pubic and axillary hair.
Menarche: First menstrual period; requires a minimum body fat percentage.
Climacteric and Menopause
Physiological Changes
Climacteric refers to the midlife decline in reproductive hormones due to depletion of ovarian follicles, culminating in menopause (cessation of menstruation, average age 52). This results in atrophy of reproductive organs, decreased bone mass, increased cardiovascular risk, and hot flashes. Hormone replacement therapy (HRT) may be used to manage symptoms.
Oogenesis and Follicle Development
Oocyte Maturation
By puberty, the ovaries contain approximately 400,000 oocytes. FSH and LH stimulate the maturation of follicles, each lined with granulosa cells. The process of oogenesis continues from puberty to menopause.
Menstrual Cycle
Phases and Hormonal Control
The menstrual cycle averages 28 days and is regulated by a hierarchy of hormonal control: hypothalamus → pituitary → ovaries → uterus. It consists of two main phases: the follicular phase and the luteal phase.
Follicular phase (days 1-14): Follicles grow, and the endometrium is rebuilt. Estrogen is secreted by the dominant follicle.
Ovulation (day 14): Triggered by an LH surge, the mature follicle ruptures and releases the oocyte.
Luteal phase (days 15-28): The corpus luteum forms and secretes progesterone, stimulating endometrial thickening. If pregnancy does not occur, the corpus luteum degenerates, and the endometrium is shed.
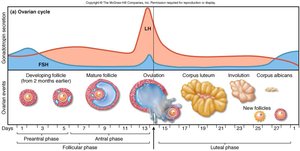
Ovulation
Ovulation is the release of the oocyte from the mature follicle, typically occurring around day 14 of the cycle. It is preceded by a surge in LH, which causes the follicle to rupture. The fimbriae of the uterine tube help capture the oocyte, and cilia move it toward the uterus. Basal body temperature rises slightly after ovulation.

Hormonal Regulation: Pituitary-Ovarian Axis
The pituitary-ovarian axis describes the feedback loop between the hypothalamus, pituitary gland, and ovaries. GnRH from the hypothalamus stimulates the pituitary to release FSH and LH, which regulate follicle development and hormone secretion in the ovaries.

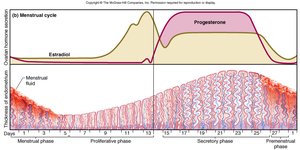
Endometrial Changes
The endometrium undergoes cyclic changes in response to ovarian hormones:
Proliferative phase: Endometrial tissue is rebuilt (mitosis).
Secretory phase: Further thickening due to secretion and fluid accumulation.
Menstrual phase: Blood, serous fluid, and endometrial tissue are discharged due to vasoconstriction and ischemia of the functional layer.
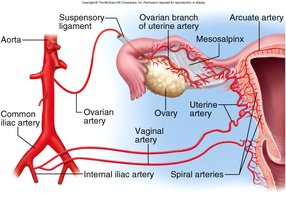
Blood Supply and Vessels of the Reproductive Tract
The reproductive tract receives blood from branches of the internal iliac artery, including the uterine, vaginal, and ovarian arteries. Hormonal changes cause spiral artery vasoconstriction, leading to necrosis of the functional layer and menstrual flow.
Contraception
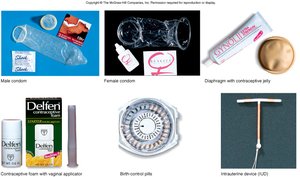
Contraceptive Devices
Various contraceptive methods are available, including barrier methods (condoms, diaphragms), hormonal methods (pills, injections), intrauterine devices (IUDs), and emergency contraception. Each method has different mechanisms and effectiveness rates.
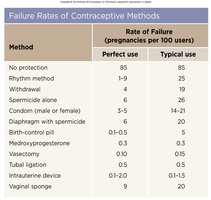
Failure Rates of Contraceptive Methods
The effectiveness of contraceptive methods is measured by the rate of failure (pregnancies per 100 users per year). Methods such as IUDs and hormonal pills have lower failure rates compared to barrier methods or no protection.
Method | Perfect Use | Typical Use |
|---|---|---|
No protection | 85 | 85 |
Rhythm method | 1-9 | 25 |
Withdrawal | 4 | 19 |
Spermicide alone | 6 | 26 |
Condom (male or female) | 3-5 | 14-20 |
Diaphragm with spermicide | 1-2 | 6 |
Birth-control pill | 0.1-0.5 | 3 |
Medroxyprogesterone | 0.3 | 0.3 |
Vasectomy | 0.1 | 0.15 |
Tubal ligation | 0.5 | 0.5 |
Intrauterine device | 0.2-0.9 | 0.7-1.5 |
Vaginal sponge | 9 | 20 |
Emergency Contraception
Emergency contraceptive pills (ECPs), such as Plan B (levonorgestrel), are high-dose hormone pills taken within 72 hours of unprotected intercourse. They work by inhibiting ovulation, altering sperm or egg transport, and preventing implantation of a blastocyst.

