 Back
BackThe Male Reproductive System: Structure, Function, and Clinical Aspects
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Overview of the Male Reproductive System
Primary and Secondary Sex Organs
The male reproductive system is composed of primary and secondary sex organs, each with distinct roles in reproduction.
Primary sex organs (gonads): The testes produce sperm cells (male gametes) and secrete sex hormones.
Secondary sex organs: These include the ducts (epididymis, ductus deferens, ejaculatory duct, urethra), glands (seminal vesicles, prostate, bulbourethral glands), and the penis, which are involved in the transport and delivery of sperm.
Secondary sex characteristics: Features that develop at puberty to attract a mate, such as pubic, axillary, and facial hair, scent glands, body morphology, and a low-pitched voice in males.

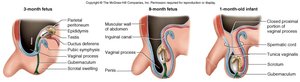
Development of External Genitalia
Embryological Differentiation
Male and female external genitalia develop from the same embryonic structures, known as homologous structures. Differentiation is typically complete by week 12 of gestation.
Homologous structures: For example, the penis in males and the clitoris in females originate from the same embryonic tissue.
Disorders: Excess androgens during fetal development can cause abnormal enlargement of the clitoris.

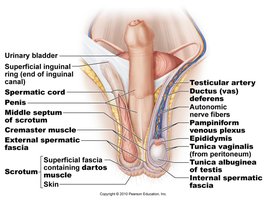
Anatomy of the Male Inguinal and Scrotal Region
Key Structures
The inguinal and scrotal regions contain essential structures for sperm production and transport.
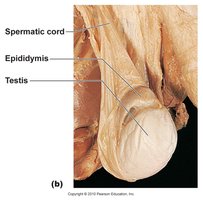
Testis: The primary reproductive organ, located within the scrotum.
Spermatic cord: Contains the ductus (vas) deferens, testicular artery, veins, nerves, and lymphatics.
Epididymis: Site of sperm maturation and storage.
Penis and scrotum: External genitalia involved in copulation and protection of the testes.
Descent of the Testes
Process and Clinical Significance
The testes develop near the kidneys and descend into the scrotum via the inguinal canal, a process essential for normal sperm production due to temperature regulation.
Timing: Descent begins at weeks 6-10 of gestation and is usually complete by week 28.
Cryptorchidism: About 3% of boys are born with undescended testes, which may require medical intervention.
Temperature regulation: The scrotal location keeps the testes cooler than core body temperature, which is necessary for spermatogenesis.
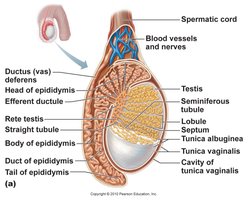
Testes: Structure and Function
Internal Anatomy
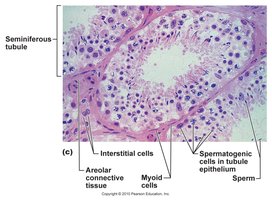
The testes are composed of seminiferous tubules, where sperm are produced, and interstitial cells, which secrete testosterone.
Seminiferous tubules: Lined with germinal epithelium for sperm production.
Interstitial (Leydig) cells: Located between tubules, responsible for testosterone production.
Sustentacular (Sertoli) cells: Support and nourish developing sperm; form the blood-testis barrier to protect sperm from the immune system.
Testicular Thermoregulation
Mechanisms for Temperature Control
Sperm production requires a temperature lower than core body temperature. The pampiniform plexus acts as a countercurrent heat exchanger to cool arterial blood entering the testis.
Pampiniform plexus: Network of veins that cools the blood before it reaches the testes.
Importance: Maintains optimal temperature for spermatogenesis.

Testicular Cancer
Clinical Features
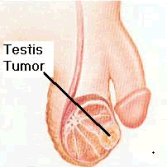
Testicular cancer is the most common solid tumor in men aged 15-35 years. Early detection through self-examination is critical for a high cure rate.
Symptoms: Painless lump or enlargement of the testis.
Prognosis: Highly curable if detected early.
Inguinal Hernia
Definition and Clinical Importance
An inguinal hernia occurs when a portion of the small intestine enters the inguinal canal through a weak area in the abdominal wall fascia.
Symptoms: Bulge in the groin, discomfort, or pain, especially when lifting or straining.
Clinical significance: May require surgical repair to prevent complications.

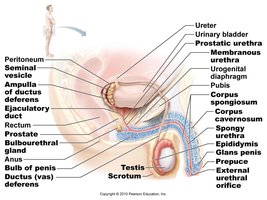
Male Duct System
Pathway of Sperm
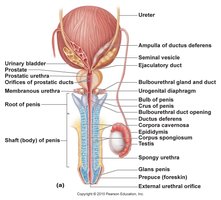
Sperm travel through a series of ducts from the testes to the external environment.
Epididymis: Site of sperm maturation and storage; sperm remain fertile for about 60 days.
Ductus (vas) deferens: Transports sperm from the epididymis to the ejaculatory duct.
Ejaculatory duct: Formed by the union of the ductus deferens and seminal vesicle; passes through the prostate to empty into the urethra.
Urethra: Conveys both urine and semen (at different times); the spongy urethra is the internal portion leading to the external urethral orifice.
Accessory Glands
Seminal Vesicles, Prostate, and Bulbourethral Glands
Accessory glands produce seminal fluid, which nourishes and protects sperm.
Seminal vesicles: Contribute about 60% of semen volume; secrete fructose and other substances for sperm energy and motility.
Prostate gland: Surrounds the urethra and ejaculatory duct; contributes about 30% of semen volume; secretes enzymes and prostate-specific antigen (PSA).
Bulbourethral (Cowper’s) glands: Secrete lubricating fluid that neutralizes acidity of residual urine in the urethra.
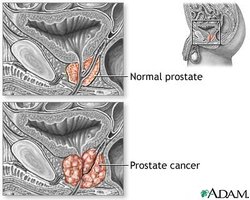
Prostate Gland: Clinical Aspects
Benign Prostatic Hyperplasia and Prostate Cancer
The prostate gland remains the same size until after age 45, after which benign prostatic hyperplasia (BPH) is common. Prostate cancer is the second most common cancer in men.
BPH: Noncancerous enlargement of the prostate, common in older men.
Prostate cancer: Diagnosed by rectal exam and/or PSA testing; treatments may affect sexual function.
Penis: Structure and Clinical Considerations
Anatomy and Function
The penis is the copulatory organ that allows for internal fertilization. The prepuce (foreskin) covers the glans and may be removed during circumcision.
Prepuce (foreskin): Removal (circumcision) is associated with decreased risk of certain STDs and penile cancer.
Glans: The sensitive tip of the penis.

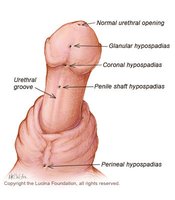
Hypospadias
Hypospadias is a common birth defect where the urethral opening is located on the underside of the penis rather than at the tip. It is usually corrected surgically in infancy.
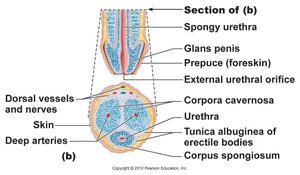
Internal Structure of the Penis
The penis contains three cylindrical bodies of erectile tissue: one corpus spongiosum (ventral) and two corpora cavernosa (dorsal), which fill with blood during arousal to produce an erection.
Corpus spongiosum: Surrounds the urethra and prevents it from pinching closed during erection.
Corpora cavernosa: Main erectile bodies responsible for penile rigidity.
Cell Division: Mitosis and Meiosis
Comparison and Significance
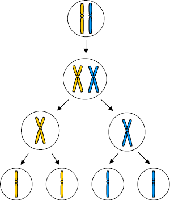
Mitosis and meiosis are two types of cell division. Mitosis produces genetically identical cells for growth and repair, while meiosis produces gametes with half the chromosome number for sexual reproduction.
Mitosis: One cell division; produces two diploid (2n) cells.
Meiosis: Two cell divisions (one DNA replication); produces four haploid (n) gametes, maintaining chromosome number across generations.
Spermatogenesis and Spermiogenesis
Stages of Sperm Development
Spermatogenesis is the process of sperm cell formation, beginning with spermatogonia and ending with mature spermatozoa. Spermiogenesis is the final stage, where spermatids transform into spermatozoa.
Spermatogonium: Stem cell that divides by mitosis.
Primary spermatocyte: Undergoes meiosis I to form secondary spermatocytes.
Secondary spermatocytes: Undergo meiosis II to form spermatids.
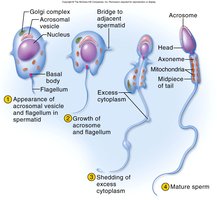
Spermiogenesis: Spermatids discard excess cytoplasm and develop tails to become spermatozoa.


Spermatozoan Structure
Functional Anatomy
The mature sperm cell consists of a head, midpiece, and tail, each specialized for fertilization.
Head: Contains the haploid nucleus and acrosome (enzymes for egg penetration).
Midpiece: Packed with mitochondria to provide ATP for motility.
Tail (flagellum): Propels the sperm.

Semen Composition and Function
Components and Roles
Semen is a mixture of sperm and secretions from accessory glands. It provides nutrients, protection, and a medium for sperm transport.
Volume: 2-5 mL per ejaculation; normal sperm count is 50-120 million/mL.
Key components: Fructose (energy), fibrinogen (clotting), enzymes (liquefaction), prostaglandins (stimulate female contractions), spermine (pH stabilization).
Infertility: Defined as sperm count less than 20 million/mL.
Puberty and Endocrine Control
Hormonal Regulation
Puberty is initiated by a surge of pituitary gonadotropins, leading to the development of secondary sexual characteristics and reproductive capability.
GnRH (gonadotropin-releasing hormone): Produced by the hypothalamus; stimulates the anterior pituitary.
LH (luteinizing hormone): Stimulates interstitial cells to produce testosterone.
FSH (follicle-stimulating hormone): Stimulates sustentacular cells to promote spermatogenesis.
Testosterone: Effects and Aging
Physiological Roles and Age-Related Changes
Testosterone is responsible for the development and maintenance of male secondary sexual characteristics, libido, and spermatogenesis. Levels peak in early adulthood and decline with age.
Secondary sexual organs: Enlargement and functional maturation.
Other effects: Increased muscle mass, erythropoiesis, and libido.
Aging: Decline in testosterone leads to symptoms such as mood changes and erectile dysfunction.
Erectile Dysfunction (ED)
Causes and Treatment
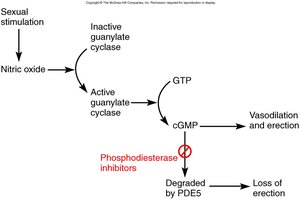
ED is the inability to maintain an erection, often due to deficient nitric oxide release. Causes include aging, hormonal decline, cardiovascular and neurological diseases, diabetes, medications, and psychological factors.
Treatment: Phosphodiesterase inhibitors (e.g., Viagra, Levitra, Cialis) enhance the nitric oxide pathway to promote erection.
Sexually Transmitted Diseases (STDs)
Bacterial and Viral Infections
STDs can affect the male reproductive system, leading to complications such as infertility and cancer.
Type | Examples | Key Features |
|---|---|---|
Bacterial | Chlamydia, Gonorrhea, Syphilis | Often curable with antibiotics; can cause infertility and pelvic inflammatory disease (PID) |
Viral | Herpes Simplex Virus (HSV-II), Human Papilloma Virus (HPV), AIDS | Chronic, may cause recurrent symptoms or cancer (HPV) |
Chlamydia
Incubation: 1-3 weeks; symptoms include watery discharge and testicular pain.
Complications: Infertility in women due to fallopian tube scarring; often co-occurs with gonorrhea.
Treatment: Antibiotics.
Gonorrhea
Symptoms in males: Painful urination, pus-filled discharge.
Symptoms in females: May be asymptomatic or present with discharge and urethritis.
Complications: PID and infertility; treated with antibiotics.
Syphilis
Stages: Primary (chancre), secondary, and tertiary (can cause dementia and cardiovascular damage).
Treatment: Antibiotics; early detection is crucial.

Genital Herpes
Cause: Herpes Simplex Virus (HSV-II); related to HSV-I (cold sores).
Symptoms: Painful blisters, relapses common, contagious even without ulcers.
Genital Warts (HPV)
Cause: Human Papilloma Virus (HPV); most common STD.
Complications: Major risk factor for cervical and penile cancer.
Treatment: Lesions treated with freezing or lasers.

