 Back
BackThe Respiratory System: Lungs, Pleurae, and Pulmonary Ventilation
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Gross Anatomy of the Lungs and Pleurae
Overview of Lung Structure
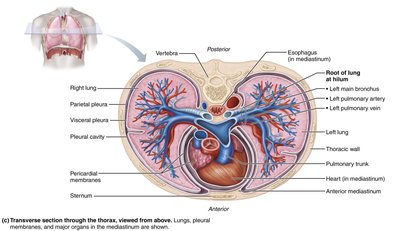
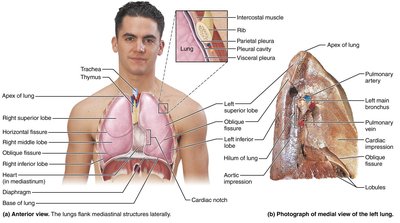
The lungs are paired organs located in the thoracic cavity, flanking the mediastinum. They are responsible for gas exchange and are connected to the mediastinum by the root, which contains bronchi, blood vessels, lymphatics, and nerves.
Apex: The narrow superior tip of each lung.
Base: The broad inferior surface resting on the diaphragm.
Hilum: The medial entry/exit site for bronchi, blood vessels, lymphatics, and nerves.
Anatomical Differences Between Right and Left Lungs
The right and left lungs differ in the number of lobes and the presence of specific anatomical features.
Right Lung: Three lobes (superior, middle, inferior) separated by horizontal and oblique fissures.
Left Lung: Two lobes (superior, inferior) separated by an oblique fissure; contains the cardiac notch to accommodate the heart.
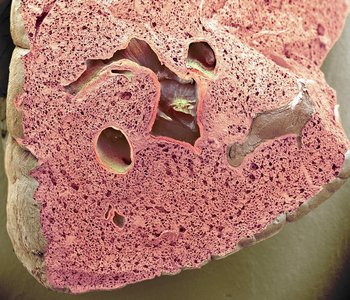
Lung Tissue and Stroma
The lungs are composed mostly of air spaces, with the remainder being the stroma—elastic connective tissue that provides stretch and recoil properties essential for ventilation.
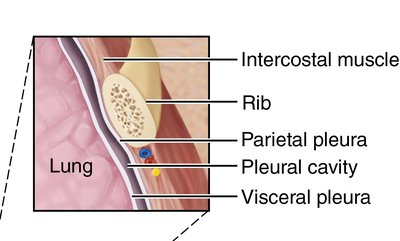
Pleurae of the Lungs
Each lung is enclosed by a double-layered serous membrane called the pleura:
Parietal pleura: Lines the thoracic wall and superior diaphragm.
Visceral pleura: Covers the external lung surface.
Pleural cavity: The space between the layers, filled with pleural fluid to reduce friction and create surface tension, helping the lungs adhere to the thoracic wall.
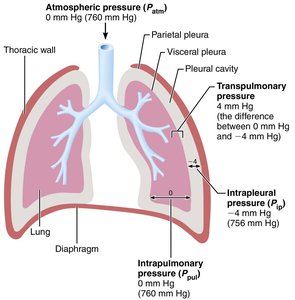
Pressure Relationships and Pulmonary Ventilation
Key Pressures in the Thoracic Cavity
Three main pressures are involved in breathing:
Atmospheric Pressure (Patm): Pressure exerted by air outside the body (760 mmHg at sea level).
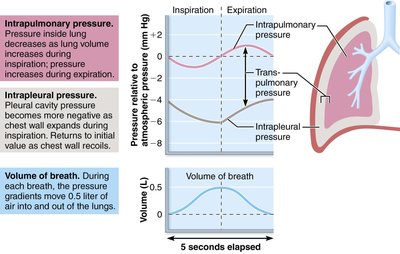
Intrapulmonary Pressure (Ppul): Pressure within the alveoli; fluctuates with breathing but always equalizes with atmospheric pressure.
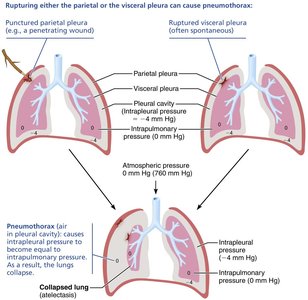
Intrapleural Pressure (Pip): Pressure within the pleural cavity; always negative relative to Ppul (about -4 mmHg).
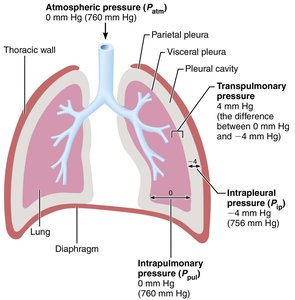
Transpulmonary Pressure
Transpulmonary pressure is the difference between intrapulmonary and intrapleural pressures (Ppul - Pip). It keeps the lungs inflated; if this pressure is lost, the lungs collapse.
Example:
Homeostatic Imbalance: Pneumothorax and Atelectasis
If air enters the pleural cavity (pneumothorax), the pressure equalizes with atmospheric pressure, causing lung collapse (atelectasis). This can result from trauma or disease and is treated by removing the air/fluid and sealing the wound.
Mechanics of Pulmonary Ventilation
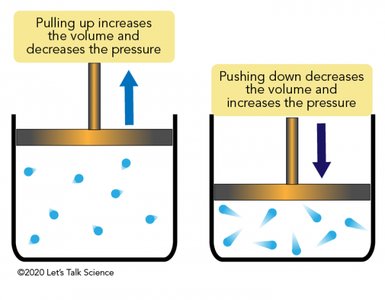
Boyle's Law and Breathing
Breathing is driven by pressure changes resulting from volume changes in the thoracic cavity, described by Boyle's Law:
As volume increases, pressure decreases.
As volume decreases, pressure increases.
Mathematically:
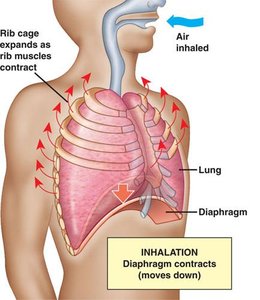
Inspiration (Inhalation)
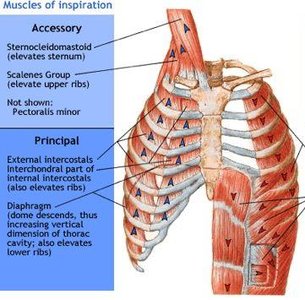
Inspiration is an active process requiring muscle contraction:
Diaphragm: Contracts and flattens, increasing thoracic volume.
External intercostals: Elevate the ribs, expanding the thoracic cavity.
Result: Ppul drops below Patm, and air flows into the lungs.
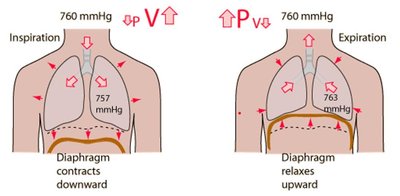
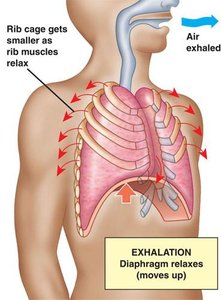
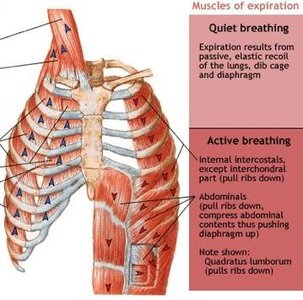
Expiration (Exhalation)
Expiration is usually passive, relying on the elastic recoil of the lungs and relaxation of inspiratory muscles. Forced expiration is active, involving abdominal and internal intercostal muscles.
As thoracic volume decreases, Ppul rises above Patm, and air flows out.
Pressure Changes During Breathing
During each breath, intrapulmonary and intrapleural pressures fluctuate, creating pressure gradients that move air in and out of the lungs.
Physical Factors Influencing Pulmonary Ventilation
Airflow, Pressure, and Resistance
Airflow into and out of the lungs is governed by the relationship:
Flow () is directly proportional to the pressure gradient () and inversely proportional to resistance ():
Resistance is mainly determined by airway diameter; smaller bronchioles increase resistance.
Lung Compliance
Lung compliance refers to the ease with which the lungs can be expanded. High compliance means the lungs expand easily; low compliance makes breathing more difficult. Determined by:
Distensibility of lung tissue (elastic fibers)
Low alveolar surface tension (due to surfactant)
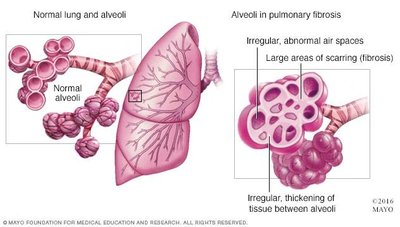
Homeostatic Imbalance: Decreased Compliance
Conditions such as pulmonary fibrosis (scarring) or decreased surfactant production reduce lung compliance, making breathing more difficult.
Measuring Pulmonary Volumes and Capacities
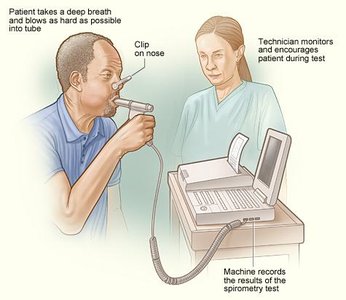
Spirometry and Lung Volumes
A spirometer is used to measure the volume of air inhaled and exhaled by the lungs. Key volumes and capacities include:
Tidal Volume (TV): Volume of air inhaled or exhaled during quiet breathing.
Inspiratory Reserve Volume (IRV): Additional air that can be inhaled after a normal inspiration.
Expiratory Reserve Volume (ERV): Additional air that can be exhaled after a normal expiration.
Vital Capacity (VC): Maximum amount of air that can be exhaled after a maximum inhalation.
Formulas:
Dead Space
Dead space refers to air that remains in the conducting airways and does not participate in gas exchange.
Pulmonary Function Tests
Pulmonary function tests help assess ventilation efficiency and diagnose respiratory disorders by measuring lung volumes, capacities, and flow rates.
