 Back
BackThe Respiratory System: Structure, Function, and Clinical Relevance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Respiratory System
Overview of the Respiratory System
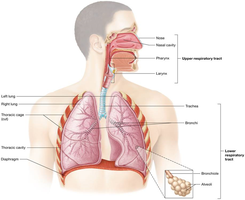
The respiratory system is responsible for supplying the body with oxygen (O2) and removing carbon dioxide (CO2), a waste product of metabolism. It is divided into upper and lower respiratory tracts, each with specialized structures and functions.
Upper respiratory tract: Includes passageways from the nose to the larynx.
Lower respiratory tract: Includes passageways from the trachea to the alveoli.
Gas exchange occurs only in the alveoli of the lungs.
Passageways purify, humidify, and warm incoming air.
Anatomy of the Respiratory System
The Nose
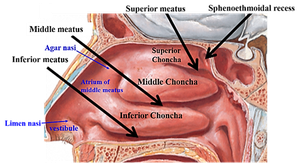
The nose is the only externally visible part of the respiratory system. It contains olfactory receptors and is lined with respiratory mucosa that warms, humidifies, and filters incoming air. The conchae are projections from the lateral walls that increase surface area and air turbulence, trapping inhaled particles. The uvula forms the inferior border and prevents food or liquid from entering the nasal cavity during swallowing.
The Pharynx
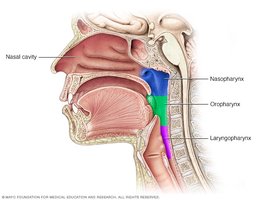
The pharynx, or throat, is a muscular passageway from the nasal cavity to the larynx. It is divided into three regions:
Nasopharynx: Superior region behind the nasal cavity.
Oropharynx: Middle region behind the mouth.
Laryngopharynx: Inferior region attached to the larynx.
The oropharynx and laryngopharynx serve as common passageways for air and food and are lined with nonkeratinized stratified squamous epithelium. The epiglottis routes food into the esophagus.
The Larynx
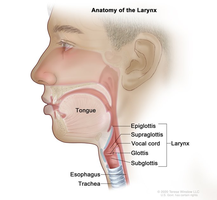
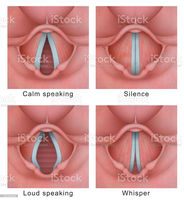
The larynx, or voice box, is located below the pharynx. It routes air and food into proper channels and is made of 8 rigid hyaline cartilages, with the thyroid cartilage (Adam’s apple) being the largest. The vocal folds (true vocal cords) vibrate with expelled air to allow speech, while the false vocal cords (vestibular folds) do not produce sound. The glottis includes the vocal cords and the opening between them. The epiglottis is a flap of elastic cartilage that covers the larynx during swallowing.

The Trachea and Bronchial Tree
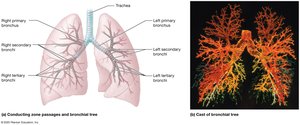
The trachea, or windpipe, is a 4-inch-long tube that connects to the larynx and is reinforced with C-shaped rings of hyaline cartilage to keep it open. It is lined with ciliated mucosa that expels mucus loaded with dust and debris away from the lungs. The trachea branches into the right and left primary bronchi, which further divide into secondary and tertiary bronchi, bronchioles, and terminal bronchioles, forming the bronchial tree.
The Lungs
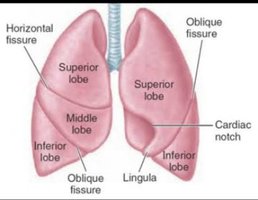
The lungs occupy the thoracic cavity except for the central mediastinum. The apex is near the clavicle, and the base rests on the diaphragm. The hilum is the region where bronchi, blood vessels, lymphatics, and nerves enter and exit the lung. The right lung has three lobes, and the left lung has two lobes.
Histology of the Respiratory Tract
The mucosa of the trachea consists of pseudostratified ciliated columnar epithelium with goblet cells. The conducting zone includes all passageways from the nasal tract to the terminal bronchioles, while the respiratory zone includes respiratory bronchioles, alveolar ducts, alveolar sacs, and alveoli—the only site of gas exchange.
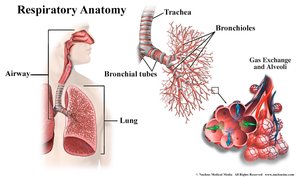
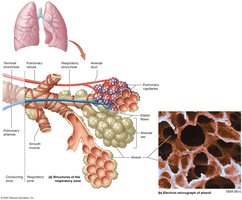
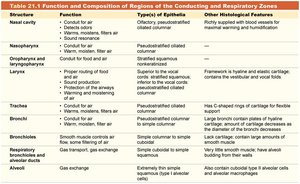
Table: Function and Composition of Regions of the Conducting and Respiratory Zones
Structure | Function | Type(s) of Epithelia | Other Histological Features |
|---|---|---|---|
Nasal cavity | Conduit for air; warms, moistens, filters air | Olfactory, pseudostratified ciliated columnar | Richly supplied with blood vessels and mucous glands |
Nasopharynx | Conduit for air | Pseudostratified ciliated columnar | — |
Oropharynx and laryngopharynx | Conduit for food and air | Stratified squamous | — |
Larynx | Proper routing of food and air; sound production | Stratified squamous (superior); pseudostratified ciliated columnar (inferior) | Framework is hyaline and elastic cartilage; contains vocal folds |
Trachea | Conduit for air; filters, moistens air | Pseudostratified ciliated columnar | Has C-shaped rings of cartilage for flexibility |
Bronchi | Conduit for air; filters, moistens air | Pseudostratified ciliated columnar | Large bronchi contain plates of hyaline cartilage; smooth muscle increases as bronchi get smaller |
Bronchioles | Conduit for air; gas exchange | Simple columnar to simple cuboidal | Large amounts of smooth muscle; little cartilage |
Respiratory bronchioles, alveolar ducts, alveoli | Gas exchange | Extremely thin simple squamous (Type I alveolar cells) | Alveolar macrophages; surfactant-secreting cells |
The Respiratory Membrane and Alveoli
The respiratory membrane (air-blood barrier) consists of alveolar and capillary walls with fused basement membranes. Gas exchange occurs by diffusion: O2 enters the blood, and CO2 enters the alveoli. Alveolar macrophages provide protection, and surfactant (produced by Type II pneumocytes) reduces surface tension, preventing alveolar collapse.
Type I pneumocytes: Squamous epithelial cells, permit gas exchange by diffusion, compose 90% of alveolar surface.
Type II pneumocytes: Produce surfactant, compose 10% of alveolar surface.
Mechanics of Breathing (Pulmonary Ventilation)
Phases of Pulmonary Ventilation
Pulmonary ventilation is the process of moving air in and out of the lungs. It depends on volume changes in the thoracic cavity, which lead to pressure changes and cause a flow of gases to equalize pressure.
Inspiration (inhalation): Diaphragm and external intercostal muscles contract (active process), increasing intrapulmonary volume and decreasing gas pressure, causing air to flow into the lungs.
Expiration (exhalation): Diaphragm and internal intercostal muscles relax (passive process), decreasing intrapulmonary volume and increasing gas pressure, causing air to flow out of the lungs.
Forced expiration: Occurs by contraction of internal intercostal muscles to depress the rib cage.
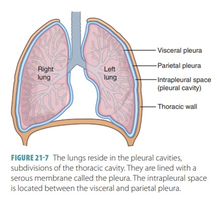
Intrapleural pressure: Always negative; if it equals atmospheric pressure, lungs will collapse.
Respiratory Volumes and Capacities
Measurement and Definitions
Respiratory volumes and capacities are measured with a spirometer and are affected by size, sex, age, and physical condition. Capacities are calculated using two or more volumes.
Tidal Volume (TV): Volume of air inhaled or exhaled in a normal breath.
Inspiratory Reserve Volume (IRV): Additional air that can be inhaled after a normal inspiration.
Expiratory Reserve Volume (ERV): Additional air that can be exhaled after a normal expiration.
Residual Volume (RV): Air remaining in the lungs after forced expiration.
Vital Capacity (VC):
Total Lung Capacity (TLC):
Alveolar Ventilation Rate (AVR): where is tidal volume, is dead space, and is respiratory rate per minute.
Gas Exchange and Transport
Events of Respiration
Pulmonary ventilation: Moving air in and out of the lungs.
External respiration: Gas exchange between alveoli and pulmonary blood.
Respiratory gas transport: Transport of O2 and CO2 via blood.
Internal respiration: Gas exchange between blood and tissues in systemic capillaries.
Gas Exchange Mechanisms
O2 diffuses from alveoli to pulmonary capillaries; CO2 diffuses from blood to alveoli.
O2 is transported mainly bound to hemoglobin as oxyhemoglobin (HbO2).
CO2 is transported mainly as bicarbonate ion (HCO3–) in plasma, and also as carbaminohemoglobin and dissolved in plasma.
Chloride shift: Cl– moves into RBCs as HCO3– moves out.
Gas Laws Affecting Respiration
Dalton’s Law of Partial Pressures: Each gas in a mixture exerts its own pressure; total pressure is the sum of partial pressures.
Henry’s Law: The amount of gas that dissolves in a liquid is proportional to its partial pressure and solubility.
Factors Affecting Hemoglobin-Oxygen Affinity
Increased temperature, acidity (Bohr effect), pCO2, and BPG decrease hemoglobin’s affinity for O2, facilitating unloading to tissues.
BPG increases at high altitude and with increased metabolism, promoting O2 release.
Control of Respiration
Neural and Chemical Regulation
Respiratory centers in the medulla and pons regulate rate and depth of breathing.
CO2 levels are the most important stimulus for breathing; detected by central chemoreceptors in the medulla.
O2 levels are detected by peripheral chemoreceptors in the aorta and carotid arteries.
Non-neural factors: Physical activity, temperature, emotions, and volition can influence breathing.
Respiratory Disorders
Chronic Obstructive Pulmonary Disease (COPD)
Includes chronic bronchitis and emphysema; most patients have a history of smoking.
Symptoms: Labored breathing, coughing, frequent infections, hypoxia, CO2 retention, respiratory acidosis, and respiratory failure.
Asthma
Airways are hyperresponsive to triggers (allergens, exercise, pollutants).
Bronchoconstriction, inflammation, and thick mucus increase airway resistance.
Treatment: Bronchodilators and anti-inflammatory steroids.
Chronic Bronchitis
Inflammation of lower respiratory mucosa; excessive mucus impairs ventilation and gas exchange.
Patients may become cyanotic (“blue bloaters”).
Emphysema
Alveolar walls collapse, reducing surface area; lungs lose elasticity.
Patients require more energy to exhale and may develop a barrel chest (“pink puffers”).
Influenza and COVID-19
Influenza is caused by viruses; symptoms include inflammation, increased mucus, and destruction of epithelial cells.
COVID-19 (SARS-CoV-2) can cause severe respiratory distress, especially in high-risk individuals. It infects respiratory epithelial cells, particularly Type II alveolar cells, and can lead to ARDS (acute respiratory distress syndrome).
Lung Cancer
Leading cause of cancer death; nearly 90% of cases are due to smoking.
Symptoms: Cough, blood-streaked sputum, chest pain, recurrent infections, and fluid accumulation.
