 Back
BackThe Urinary System: Structure, Function, and Regulation
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Urinary System
Overview and Functions
The urinary system is essential for maintaining the body's internal environment by filtering blood, removing waste, and regulating fluid and electrolyte balance. It consists of the kidneys, ureters, urinary bladder, and urethra.
Blood Filtration: Kidneys filter blood to remove metabolic wastes and toxins.
Blood Pressure Regulation: Kidneys control long-term blood pressure via the renin-angiotensin-aldosterone system (RAAS).
Acid-Base Balance: Kidneys help maintain blood pH (7.35–7.45) by excreting or reabsorbing hydrogen and bicarbonate ions.
Hormone Production: Kidneys produce erythropoietin (stimulates red blood cell production) and activate vitamin D.
Organs of the Urinary System
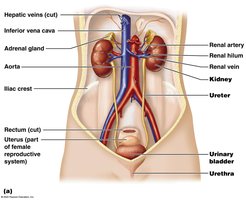
The urinary system includes two kidneys, two ureters, the urinary bladder, and the urethra. Each organ plays a specific role in urine production and excretion.
Kidneys: Filter blood and produce urine.
Ureters: Transport urine from kidneys to bladder.
Urinary Bladder: Temporarily stores urine.
Urethra: Expels urine from the body.
Kidney Structure and Location
Location and Protective Layers
The kidneys are retroperitoneal organs located on the dorsal wall of the abdomen, between vertebrae T12 and L3. The right kidney sits slightly lower due to the liver's position above it. Each kidney is protected by three layers:
Renal Capsule: Tough, fibrous connective tissue covering the kidney.
Adipose Capsule: Fatty layer that cushions the kidney.
Renal Fascia: Thin connective tissue anchoring the kidney to the abdominal wall.
Internal Anatomy of the Kidney
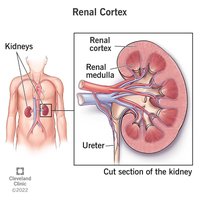
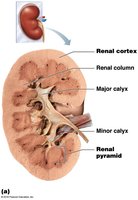
The kidney's internal structure is divided into the renal cortex (outer layer) and renal medulla (inner layer). The cortex is where blood filtration begins, while the medulla concentrates urine. Urine flows from the renal pyramids into minor calyces, then major calyces, and finally the renal pelvis, which leads to the ureter.
Blood Supply to the Kidneys
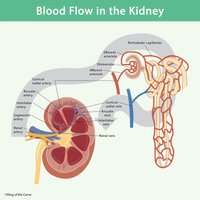
About 25% of the body's blood passes through the kidneys each minute, highlighting their importance in filtration. Blood enters via the renal artery, branches through smaller arteries, and is filtered in the glomerulus before exiting through the renal vein.

Nephron: The Functional Unit
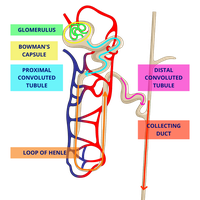
Structure of the Nephron
Each kidney contains over a million nephrons, which filter blood, reabsorb essential substances, and secrete wastes. The nephron consists of the glomerulus, Bowman's (glomerular) capsule, proximal convoluted tubule (PCT), loop of Henle, distal convoluted tubule (DCT), and collecting duct.
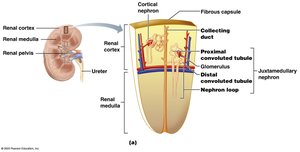
Renal Tubule and Associated Capillaries
The renal tubule processes filtrate into urine through three main sections:
Proximal Convoluted Tubule (PCT): Reabsorbs nutrients, water, and ions.
Loop of Henle: Concentrates urine by reabsorbing water and salts.
Distal Convoluted Tubule (DCT): Regulates electrolyte and pH balance, final adjustments before urine enters the collecting duct.
Peritubular capillaries surround the tubule, facilitating reabsorption and secretion.
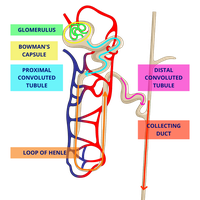
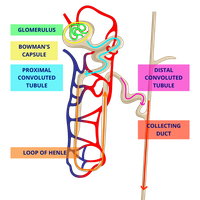
Flow of Filtrate Through the Nephron
Filtrate flows through the nephron in the following order:
Glomerular Capsule (filtration begins)
Proximal Convoluted Tubule (reabsorption)
Loop of Henle
Distal Convoluted Tubule (secretion)
Collecting Duct (urine formation complete)
Urine Formation
Three Main Processes
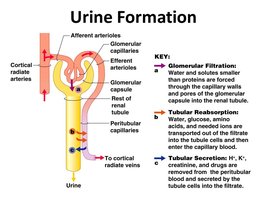
Urine formation involves three key processes:
Glomerular Filtration: Water and solutes are filtered from blood into the glomerular capsule.
Tubular Reabsorption: Useful substances (water, glucose, ions) are reabsorbed into the blood.
Tubular Secretion: Additional wastes and excess ions are secreted into the tubule for excretion.
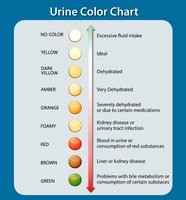
Urine Characteristics and Analysis
Normal urine is clear to pale yellow, sterile at formation, slightly acidic (pH ~6), and has a specific gravity of 1.001–1.035. It is about 95% water and 5% solutes (urea, creatinine, uric acid, electrolytes). Abnormal findings (glucose, proteins, blood cells) may indicate disease.
Urinary Tract Anatomy and Physiology
Ureters
Ureters are muscular tubes (25–30 cm long) that transport urine from the kidneys to the bladder. Kidney stones can obstruct ureters, causing pain and urinary issues.
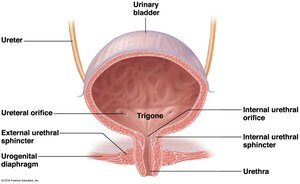
Urinary Bladder
The bladder is a muscular sac that temporarily stores urine. The trigone is a triangular area defined by the openings of the ureters and urethra. The bladder is lined with transitional epithelium, allowing expansion.
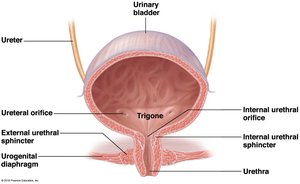
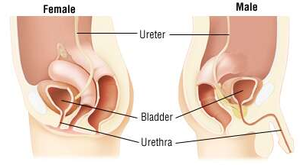
Urethra
The urethra carries urine from the bladder to the outside. In females, it is short and carries only urine; in males, it is longer and also carries sperm. Two sphincters control urine release: the internal (involuntary) and external (voluntary) urethral sphincters.
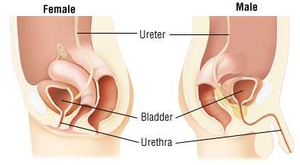
Urethra Differences and Urinary Tract Infections (UTIs)
Females have a shorter urethra, increasing the risk of UTIs. Symptoms include urgency, frequency, blood in urine, and back pain. Infections can ascend, causing cystitis or pyelonephritis.
Micturition (Voiding)
Micturition is the process of emptying the bladder. The urge to void begins when the bladder contains about 200 mL of urine. Incontinence is the loss of voluntary control, while retention is the inability to expel urine.
Water, Electrolyte, and Acid-Base Balance
Body Water Distribution
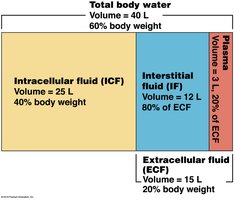
Water is vital for life, making up 50–60% of adult body weight. It is distributed in two main compartments:
Intracellular Fluid (ICF): 40% of body weight, inside cells.
Extracellular Fluid (ECF): 20% of body weight, outside cells (includes interstitial fluid and plasma).
Regulation of Water Intake and Output
Water intake comes from fluids, food, and metabolic processes. Output occurs via urine, sweat, exhaled air, and feces. The thirst mechanism, regulated by osmoreceptors in the hypothalamus, drives water intake when plasma solute concentration rises.

Hormonal Regulation of Kidney Function
Renin-Angiotensin-Aldosterone System (RAAS)
The RAAS system is activated by low blood pressure or fluid volume. Renin (from kidneys) converts angiotensinogen (from liver) to angiotensin I, which is then converted to angiotensin II by ACE. Angiotensin II causes vasoconstriction, stimulates aldosterone (increases sodium and water reabsorption), and triggers ADH release (reduces urine output).
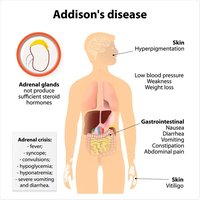
Aldosterone and Addison's Disease
Aldosterone increases sodium and water reabsorption. Addison's disease is characterized by insufficient aldosterone, leading to dehydration, low blood pressure, and electrolyte imbalance.
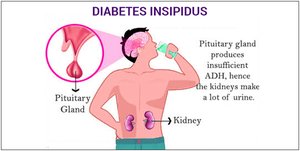
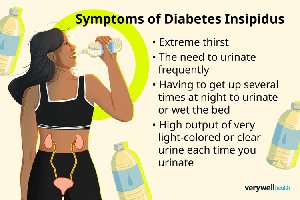
Antidiuretic Hormone (ADH) and Diabetes Insipidus
ADH reduces urine output by increasing water reabsorption. Lack of ADH causes diabetes insipidus, resulting in excessive urination and thirst.
Acid-Base Balance
Maintaining Blood pH
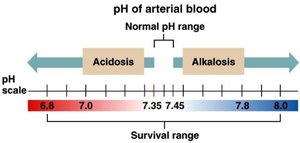
The kidneys maintain blood pH (7.35–7.45) by excreting hydrogen ions and reabsorbing bicarbonate. Imbalances can lead to acidosis (pH < 7.35) or alkalosis (pH > 7.45).
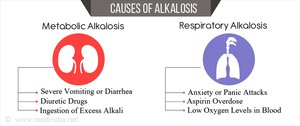
Alkalosis and Acidosis
Alkalosis occurs when blood pH is too high, often due to excessive bicarbonate or loss of CO2. Acidosis occurs when pH is too low, due to excess hydrogen ions or CO2 retention. Both conditions have metabolic and respiratory causes, with specific treatments depending on the underlying issue.
Urinary System Disorders and Development
Common Disorders
Polycystic Kidney Disease: Cyst formation obstructs urine flow.
Glomerulonephritis: Inflammation of glomeruli, often post-infection.
Kidney Stones: Hard deposits causing pain and hematuria.
UTIs: Infections affecting any part of the urinary tract.
Developmental Aspects
Fetal: Kidneys form and function by the third month; urine contributes to amniotic fluid.
Infancy: Immature kidneys, frequent urination, risk of dehydration.
Adulthood: Kidney function matures, efficient regulation of water and electrolytes.
Aging: Decline in kidney function, bladder capacity, and control; increased risk of incontinence and nocturia.
