 Back
BackThe Urinary System: Structure, Function, and Regulation
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Urinary System
Overview and Functions
The urinary system is essential for the excretion of soluble wastes and the regulation of homeostasis, including blood volume, erythrocyte production, and the removal of metabolic byproducts. The kidneys, ureters, urinary bladder, and urethra work together to filter blood, form urine, and expel it from the body.
Blood volume regulation: Kidneys adjust the volume of water excreted, influencing blood pressure and volume.
Regulation of erythrocyte production: Kidneys release erythropoietin in response to low oxygen, stimulating red blood cell production.
Urine pathway: Urine is formed in the kidneys, passes through the ureters to the urinary bladder, and is expelled via the urethra.
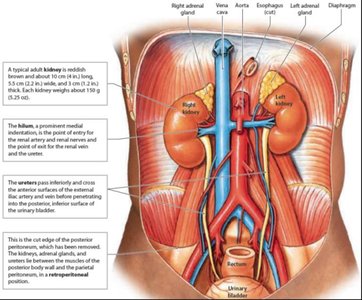
Kidney location: Retroperitoneal, just above the waist, protected by the 11th and 12th ribs (right kidney is lower).
Kidney Structure and Internal Anatomy
Gross Anatomy
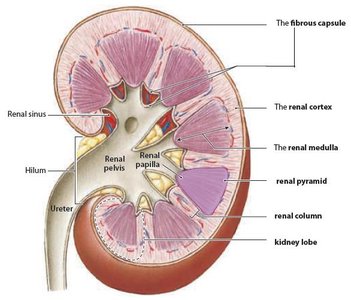
The kidneys are bean-shaped organs with distinct regions and structures that facilitate filtration and urine formation.
Renal cortex: The outer region beneath the fibrous capsule.
Renal medulla: The inner region containing 6–18 renal pyramids.
Lobe: A renal pyramid and its surrounding cortical tissue.
Renal pyramid: Conical structures extending from the cortex to the renal papilla.
Renal column: Bands of cortical tissue separating adjacent pyramids.
Renal pelvis: Collects urine from the pyramids and channels it to the ureter.
Blood and Nerve Supply
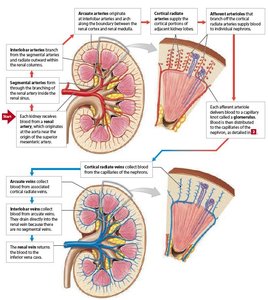
The kidneys receive a significant portion of cardiac output and are richly supplied with blood vessels and nerves.
Hilum: Entry/exit site for ureter, blood vessels, lymphatics, and nerves.
Blood supply: Kidneys receive 20–25% of cardiac output (1.2–1.3 L/min), despite being only 0.5% of body weight.
Oxygen consumption: Kidneys use about 20% of the body's oxygen.
Nephrons: The Functional Unit
Structure and Types
Nephrons are the microscopic functional units of the kidney responsible for filtering blood and forming urine. Each kidney contains about 1 million nephrons, and their number remains constant from birth.
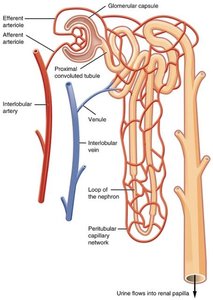
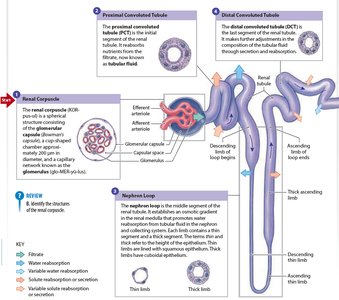
Renal corpuscle: Site of filtration (glomerulus + Bowman's capsule).
Renal tubule: Processes filtrate through reabsorption and secretion.
Nephron Processes
Glomerular filtration: Blood pressure forces water and solutes through the filtration membrane into the capsular space.
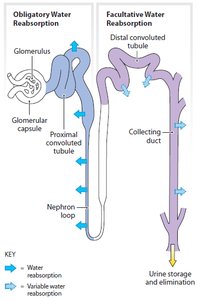
Tubular reabsorption: Returns essential substances (glucose, amino acids, 99% of water) to the blood.
Tubular secretion: Adds substances (e.g., H+, K+, creatinine) from blood into the tubular fluid for excretion.
Glomerular Filtration
Filtration Membrane and Pressure
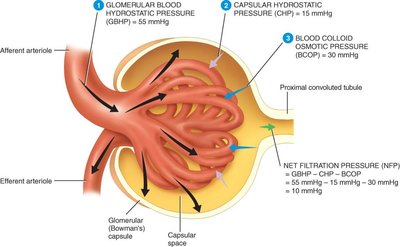
Filtration occurs across a porous membrane between the blood and the interior of the glomerular capsule. The process is driven by hydrostatic pressure and opposed by osmotic and capsular pressures.
Glomerular blood pressure (GBHP): 55 mm Hg (higher than other capillaries).
Capsular hydrostatic pressure (CHP): 15 mm Hg.
Blood colloid osmotic pressure (BCOP): 30 mm Hg.
Net filtration pressure (NFP):
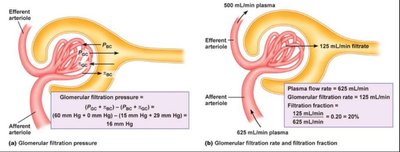
Filtration Fraction
The fraction of plasma in the afferent arterioles that becomes filtrate is called the filtration fraction, typically about 20%.
Tubular Reabsorption and Secretion
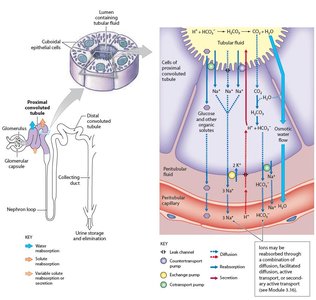
Proximal Convoluted Tubule (PCT)
The PCT reabsorbs most of the filtered nutrients, water, and ions. Microvilli increase the surface area for reabsorption, and both active and passive processes are involved.
Reabsorbs: 99% of glucose, amino acids, and other organic nutrients.
Water reabsorption: Occurs via osmosis through aquaporins.
Small proteins: Reabsorbed by pinocytosis.
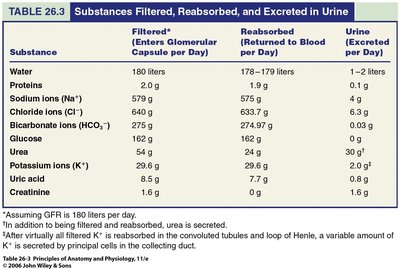
Substances Filtered, Reabsorbed, and Excreted
The table below summarizes the fate of key substances as they pass through the nephron.
Substance | Filtered (L/day) | Reabsorbed (L/day) | Excreted (L/day) |
|---|---|---|---|
Water | 180 | 178–179 | 1–2 |
Proteins | 2.0 g | 2.0 g | 0 |
Sodium ions (Na+) | 579.0 | 575.9 | 3.2 |
Chloride ions (Cl–) | 640.0 | 633.7 | 6.3 |
Bicarbonate ions (HCO3–) | 275.0 | 274.9 | 0.1 |
Glucose | 162.0 | 162.0 | 0 |
Urea | 54.0 | 24.0 | 30.0 |
Potassium ions (K+) | 29.6 | 29.6 | 2.0 |
Uric acid | 8.5 | 7.7 | 0.8 |
Creatinine | 1.6 | 0 | 1.6 |
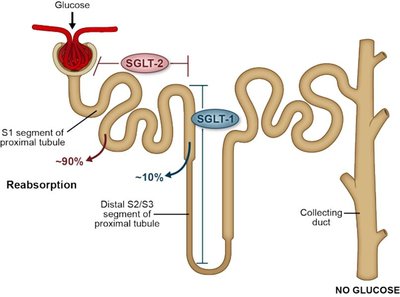
Glucose Reabsorption and Diabetes Mellitus
Normally, all filtered glucose is reabsorbed in the PCT. In diabetes mellitus, high blood glucose exceeds the renal threshold, resulting in glucose in the urine (glucosuria).
Loop of Henle (Nephron Loop)
Countercurrent Multiplication
The loop of Henle creates a concentration gradient in the medulla, allowing for water reabsorption and urine concentration.
Descending limb: Permeable to water, impermeable to solutes; water exits by osmosis.
Ascending limb: Impermeable to water; actively transports Na+ and Cl– out of the tubule.
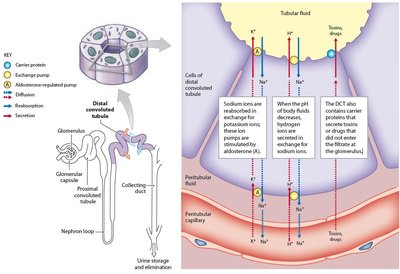
Distal Convoluted Tubule (DCT) and Collecting Duct
Reabsorption and Secretion
The DCT and collecting duct fine-tune urine composition under hormonal control (ADH, aldosterone, parathyroid hormone).
DCT: Reabsorbs Na+ (in exchange for K+ or H+), Ca2+ (stimulated by PTH), and secretes toxins/drugs.
Collecting duct: Regulates water reabsorption (ADH), Na+ reabsorption/K+ secretion (aldosterone), and acid-base balance (H+, HCO3–).
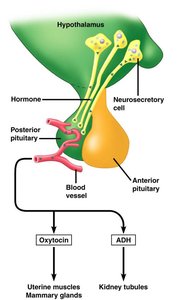
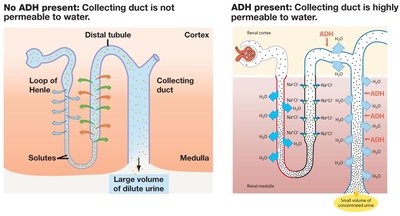
Hormonal Regulation of Urine Volume and Concentration
Antidiuretic Hormone (ADH)
ADH increases water reabsorption in the collecting duct, producing concentrated urine. In its absence, large volumes of dilute urine are formed.
Stimulus: Dehydration or increased plasma osmolarity triggers ADH release from the posterior pituitary.
Effect: Insertion of aquaporins in collecting duct cells, increasing water permeability.
Aldosterone
Aldosterone, a mineralocorticoid released by the adrenal cortex, promotes Na+ reabsorption and K+ secretion in the DCT and collecting duct. Water follows Na+ by osmosis, increasing blood volume and pressure.
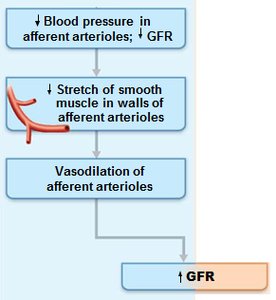
Glomerular Filtration Rate (GFR) Regulation
Intrinsic (Autoregulation) and Extrinsic Controls
GFR must remain relatively constant to ensure proper filtration. It is regulated by intrinsic (renal autoregulation) and extrinsic (neural and hormonal) mechanisms.
Intrinsic controls: Myogenic mechanism (response to blood pressure changes) and tubuloglomerular feedback (macula densa senses NaCl concentration).
Extrinsic controls: Sympathetic nervous system and renin-angiotensin-aldosterone system (RAAS) during stress or low blood pressure.

Ureters, Urinary Bladder, and Urethra
Ureters
Ureters transport urine from the renal pelvis to the urinary bladder using peristalsis, hydrostatic pressure, and gravity. They are retroperitoneal and have three layers: mucosa (transitional epithelium), muscularis (smooth muscle), and adventitia (fibrous connective tissue).
Urinary Bladder
The bladder is a hollow, muscular organ with a capacity of 700–800 mL. The trigone is a triangular region sensitive to expansion, signaling the brain when the bladder is full. The detrusor muscle contracts to expel urine.
Urethra and Sphincters
The urethra is a muscular tube with internal (involuntary) and external (voluntary) sphincters. The internal sphincter is smooth muscle at the bladder-urethra junction, while the external sphincter is skeletal muscle in the pelvic floor.
Micturition (Urination) Reflex
Neural Control
Micturition involves spinal reflexes and conscious control. The urine storage reflex is mediated by the sympathetic nervous system, while the voiding reflex is mediated by the parasympathetic system and voluntary relaxation of the external sphincter.
Urine storage reflex: Inhibits detrusor contraction and keeps the bladder closed.
Urine voiding reflex: Stretch receptors trigger detrusor contraction and sphincter relaxation.
Conscious control: The cerebral cortex can initiate or delay micturition.
Urinary Incontinence
Incontinence is the lack of voluntary control over urination, normal in infants and young children due to immature neural pathways.
Clinical Correlations
Renal Calculi (Kidney Stones)
Stones form in the renal pelvis from crystallized salts and can block the ureter, causing pain and urinary obstruction.
Hemodialysis
Hemodialysis is used in renal failure to filter wastes from the blood using a selectively permeable membrane and dialysis fluid.
Summary Table: Renal Structures and Their Functions
Segment | General Function | Specific Function |
|---|---|---|
Renal corpuscle | Filtration of plasma | Removes water and solutes from plasma |
Proximal convoluted tubule | Reabsorption of nutrients, ions, water | Active/passive reabsorption of glucose, amino acids, vitamins, ions |
Nephron loop | Reabsorption of water, Na+, Cl– | Establishes osmotic gradient in medulla |
Distal convoluted tubule | Secretion and reabsorption | Secretes ions, acids, drugs; reabsorbs Na+, Ca2+, water (hormonal control) |
Collecting system | Reabsorption/secretion of water, ions | Reabsorbs water (ADH), Na+ (aldosterone); secretes K+, H+, HCO3– |
