 Back
BackThe Urinary System: Structure, Function, and Clinical Relevance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Urinary System Overview
Introduction
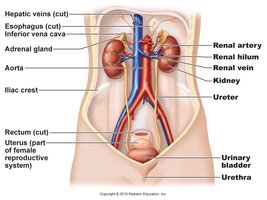
The urinary system is essential for filtering blood, removing waste, and maintaining homeostasis of water, electrolytes, and acid-base balance. It consists of the kidneys, ureters, urinary bladder, and urethra.
Kidney Anatomy and Location
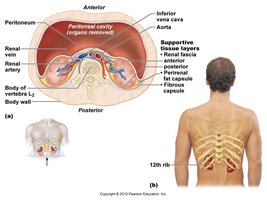
Location and Protective Structures
Location: Retroperitoneal, between T12 and L3 vertebrae.
Size: About the size of a bar of soap.
Protection: Surrounded by an adipose capsule and fibrous capsule for protection and stabilization.
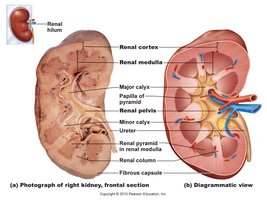
Gross Anatomy of the Kidney
Renal Cortex: Outer region containing most nephrons.
Renal Medulla: Inner region with renal pyramids and columns.
Renal Pyramid: Cone-shaped tissues in the medulla.
Renal Pelvis: Funnel-shaped structure collecting urine into the ureter.
Calyces: Minor and major calyces collect urine from pyramids.
Kidney Functions
Major Functions
Filtration: Removes waste from blood plasma.
Homeostasis: Regulates osmolarity, blood volume, blood pressure, and acid-base balance.
Secretion: Produces hormones such as renin (blood pressure regulation) and erythropoietin (stimulates RBC production).
Detoxification: Metabolizes drugs and free radicals.
Nephron Structure and Types
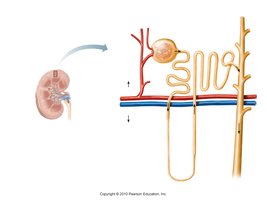
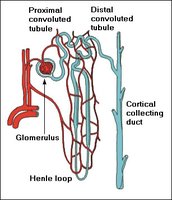
Nephron Anatomy
Nephrons are the functional units of the kidney, responsible for urine formation. Each kidney contains about 1.2 million nephrons.
Renal Corpuscle: Includes the glomerulus and Bowman’s (glomerular) capsule.
Renal Tubule: Composed of the proximal convoluted tubule (PCT), nephron loop (Loop of Henle), distal convoluted tubule (DCT), and collecting duct (CD).
Types of Nephrons
Cortical Nephrons: 85%, short loops, located near the kidney surface.
Juxtamedullary Nephrons: 15%, long loops extending deep into the medulla, crucial for concentrating urine.
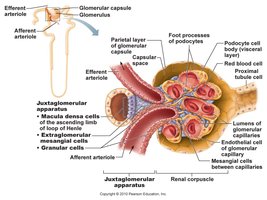
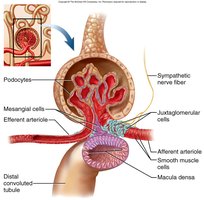
Renal Corpuscle and Filtration
Structure and Function
Glomerulus: Capillary bed where filtration occurs; high blood pressure forces small molecules through the filtration membrane.
Bowman’s Capsule: Surrounds the glomerulus and collects filtrate.
Filtration Membrane: Consists of fenestrated endothelium, basement membrane, and podocyte filtration slits; allows passage of water, electrolytes, glucose, amino acids, and small molecules, but retains large proteins and blood cells.
Renal Tubule and Urine Formation
Segments of the Renal Tubule
Proximal Convoluted Tubule (PCT): Major site of reabsorption for water, ions, and nutrients.
Nephron Loop (Loop of Henle): Descending limb reabsorbs water; ascending limb reabsorbs electrolytes (Na+, Cl-, K+).
Distal Convoluted Tubule (DCT): Further reabsorption and secretion, regulated by hormones.
Collecting Duct (CD): Final concentration of urine, regulated by ADH and aldosterone.
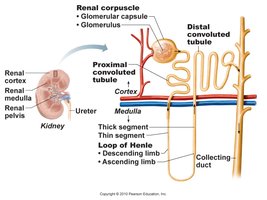
Pathway of Filtrate
glomerular capsule → PCT → nephron loop → DCT → collecting duct → minor calyx → major calyx → renal pelvis → ureter → urinary bladder → urethra
Urine Formation: Processes
Overview of Processes
Glomerular Filtration: Blood pressure forces water and solutes from glomerulus into Bowman’s capsule.
Tubular Reabsorption: Useful substances are reabsorbed from the filtrate back into the blood.
Tubular Secretion: Additional wastes are secreted from blood into the tubule.
Water Conservation: Water is reabsorbed from the collecting duct, concentrating the urine.

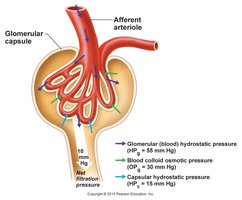
Filtration Membrane and Pressure
Filtration Membrane Structure
Fenestrated Endothelium: Pores exclude blood cells and large proteins.
Basement Membrane: Proteoglycan gel excludes large molecules.
Filtration Slits: Podocyte arms allow only small particles to pass.
Filtration Pressure
High pressure in the glomerulus (due to wider afferent arteriole) drives filtration.
Filtration pressure overrides reabsorption, ensuring continuous filtration.
Glomerular Filtration Rate (GFR) and Regulation
GFR Values and Importance
Normal GFR: ~125 mL/min (180 L/day) in males; ~105 mL/min (150 L/day) in females.
99% of filtrate is reabsorbed; only 1–2 L urine excreted per day.
High GFR: Increased urine output, risk of dehydration and electrolyte loss.
Low GFR: Anuria (low urine output), waste retention.
Regulation of GFR
Autoregulation: Myogenic mechanism and tubuloglomerular feedback stabilize GFR.
Sympathetic Control: Constriction of afferent arterioles during stress reduces GFR and urine output.
Hormonal Control: Renin-angiotensin-aldosterone system (RAAS) increases blood pressure and GFR.


Tubular Reabsorption and Secretion
Reabsorption in the PCT
Most water, ions, glucose, amino acids, and vitamins are reabsorbed in the PCT.
Peritubular capillaries have high osmolarity and low pressure, favoring reabsorption by osmosis and solvent drag.
Tubular Secretion
Removes additional wastes (urea, uric acid, ammonia, drugs) from blood into tubule.
Regulates acid-base balance by secreting H+ and bicarbonate ions.
Nephron Loop (Loop of Henle)
Descending Limb: Permeable to water, not electrolytes.
Ascending Limb: Permeable to electrolytes (Na+, Cl-, K+), not water.
Creates a salinity gradient, allowing the collecting duct to concentrate urine.

DCT and Collecting Duct
Regulated by hormones (aldosterone, ADH) for salt/water and acid/base balance.
Aldosterone increases Na+ and water reabsorption, raising blood pressure and reducing urine volume.
ADH increases water reabsorption, reducing urine volume during dehydration.

Urine Composition and Properties
Normal Characteristics
Appearance: Clear to deep amber; yellow due to urochrome.
Odor: Slightly aromatic; may change with diet or disease.
Specific Gravity: 1.005–1.030 (correlates with osmolarity).
pH: 4.5–8.2 (usually around 6.0).
Chemical Composition: 95% water, 5% solutes (urea, NaCl, KCl, creatinine, uric acid).
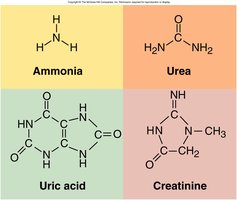
Nitrogenous Wastes
Urea: From amino acid catabolism.
Uric Acid: From nucleic acid catabolism.
Creatinine: From creatine phosphate catabolism.
Urine Volume and Disorders
Normal and Abnormal Volumes
Normal: 1–2 L/day.
Polyuria: >2 L/day (excessive urination).
Oliguria: <500 mL/day (low output).
Anuria: 0–100 mL/day (very low output).
Diabetes and Diuretics
Diabetes Mellitus: Chronic polyuria with hyperglycemia and glycosuria.
Diabetes Insipidus: ADH hyposecretion, leading to excessive dilute urine.
Diuretics: Increase urine output, used to treat hypertension and heart failure (e.g., caffeine, alcohol).

Urinary Tract Anatomy: Ureters, Bladder, and Urethra
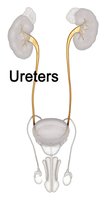
Ureters
Muscular tubes (~25 cm) transporting urine from renal pelvis to bladder by peristalsis.
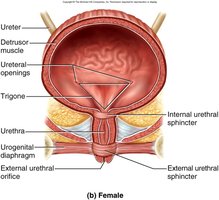
Urinary Bladder
Muscular sac for urine storage; capacity 500–800 mL.
Trigone: Triangular area between ureter and urethra openings, prone to infection.
Rugae: Folds allowing distension.
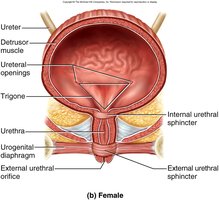
Urethra
Female: 3–4 cm, more prone to infections.
Male: 18 cm, passes through prostate and penis.
Internal Urethral Sphincter: Involuntary, smooth muscle.
External Urethral Sphincter: Voluntary, skeletal muscle.
Micturition (Voiding Urine)
Control of Urination
Bladder stretch receptors signal the micturition center when ~200 mL urine accumulates.
Results in bladder contraction and relaxation of internal sphincter; voluntary control via external sphincter.
Voluntary abdominal pressure can initiate urination if the bladder is not full.
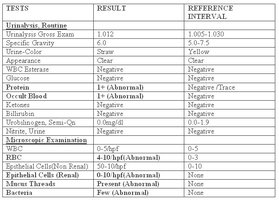
Urinalysis and Clinical Relevance
Normal and Abnormal Constituents
Normal: Urea, creatinine, uric acid, urobilinogen.
Abnormal: Albumin (albuminuria), glucose (glucosuria), blood (hematuria), pus (pyuria), ketones (ketonuria), bilirubin (bilirubinuria), microbes (UTI).

Kidney Pathology
Common Disorders
Trauma, Infection, Exercise, Hypoxia: Can cause proteinuria or hematuria.
Polycystic Kidney Disease: Genetic disorder causing multiple cysts, leading to kidney failure.
Kidney Stones (Renal Calculi): Hard granules of calcium, phosphate, uric acid, and protein; can block urine flow and cause severe pain.
Renal Insufficiency: Inability to maintain homeostasis due to nephron loss; causes include hypertension, infections, trauma, toxins, autoimmune disease, and glomerulonephritis.
Hemodialysis: Artificial filtration of blood for renal failure patients.
Renal Cell Carcinoma: Kidney cancer originating in tubule lining; symptoms include pain, abnormal urine color, and weight loss.


