 Back
BackTransport and Regulation of Respiratory Gases, and Respiratory System Disorders
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Transport of Respiratory Gases by Blood
Oxygen Transport
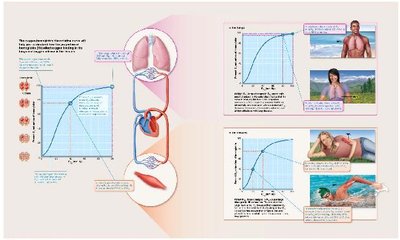
The transport of oxygen in the blood is essential for cellular respiration and energy production. Oxygen is carried in blood in two main ways:
Dissolved in plasma: About 1.5% of oxygen is transported this way.
Bound to hemoglobin (Hb): Approximately 98.5% of oxygen is loosely bound to the iron in hemoglobin within red blood cells (RBCs).
Each hemoglobin molecule consists of four polypeptide chains, each with an iron-containing heme group, allowing each Hb to carry four oxygen molecules. The combination of hemoglobin and oxygen is called oxyhemoglobin (HbO2), while hemoglobin that has released oxygen is termed reduced hemoglobin (deoxyhemoglobin, HHb).
Loading and unloading of O2 is facilitated by changes in hemoglobin's shape, which alters its affinity for oxygen. Hemoglobin can be fully saturated (all four heme groups carry O2) or partially saturated (one to three hemes carry O2).
Factors Influencing Hemoglobin Saturation
Partial pressure of oxygen (PO2): The most significant factor affecting O2 binding and release.
Temperature, blood pH, PCO2, and BPG: These factors modify hemoglobin's structure and affinity for O2.
The relationship between PO2 and hemoglobin saturation is illustrated by the oxygen-hemoglobin dissociation curve, which is S-shaped and ensures optimal oxygen pickup and delivery.
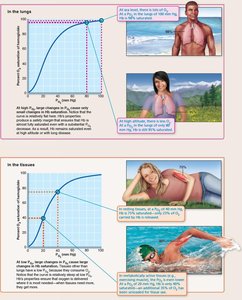
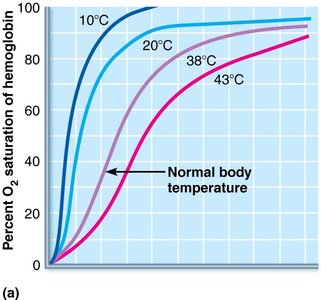
Influence of Temperature, PCO2, and Blood pH
Increases in temperature, H+, PCO2, and BPG decrease hemoglobin's affinity for O2, enhancing O2 unloading in systemic capillaries. Decreases in these factors shift the curve to the left, reducing O2 unloading.
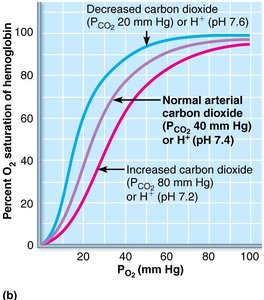
BPG is produced by RBCs during glycolysis and increases when oxygen levels are low, further promoting O2 unloading. The Bohr effect describes how declining pH and increasing PCO2 weaken the Hb-O2 bond, facilitating O2 release where needed most.
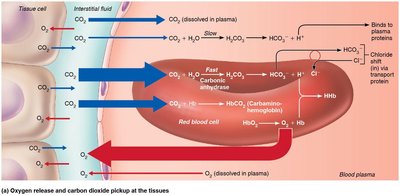
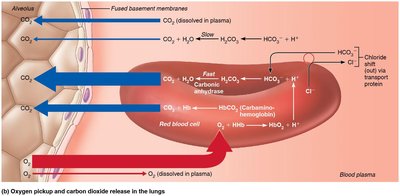
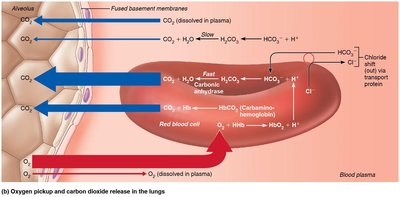
Carbon Dioxide Transport
Carbon dioxide (CO2) is transported in blood in three forms:
Dissolved in plasma: 7–10% as PCO2.
Bound to hemoglobin: Just over 20% as carbaminohemoglobin (CO2 binds to the globin part of Hb).
As bicarbonate ions (HCO3–): About 70% in plasma, formed by the reaction:
This reaction is catalyzed by the enzyme carbonic anhydrase in RBCs. The chloride shift maintains ionic balance as HCO3– leaves RBCs and Cl– enters.
Haldane Effect
The amount of CO2 transported is affected by PO2. Lower PO2 and hemoglobin O2 saturation allow more CO2 to be carried in blood. Reduced hemoglobin buffers H+ and forms carbaminohemoglobin more easily, encouraging CO2 exchange at tissues and lungs.
Influence of CO2 on Blood pH
The carbonic acid–bicarbonate buffer system helps blood resist changes in pH:
If H+ concentration rises, excess H+ is removed by combining with HCO3– to form H2CO3.
If H+ concentration drops, H2CO3 dissociates, releasing H+.
Changes in respiratory rate and depth affect blood pH, with slow, shallow breathing increasing CO2 and lowering pH, and rapid, deep breathing decreasing CO2 and raising pH.
Control of Respiration
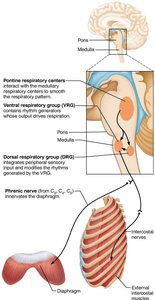
Neural Mechanisms
Respiratory rhythms are regulated by higher brain centers, chemoreceptors, and reflexes. Neural controls involve neurons in the reticular formation of the medulla and pons:
Ventral respiratory group (VRG): Rhythm-generating and integrative center; sets eupnea (normal respiratory rate and rhythm).
Dorsal respiratory group (DRG): Integrates input from peripheral stretch and chemoreceptors, then sends information to VRG neurons.
Pontine respiratory centers: Influence and modify activity of VRG, smoothing transitions between inspiration and expiration.
Factors Influencing Breathing Rate and Depth
Depth is determined by how actively the respiratory center stimulates respiratory muscles, while rate is determined by how long the center is active. Both are modified by changing body demands.
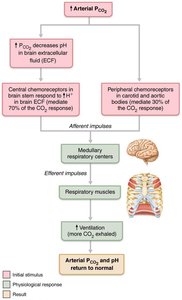
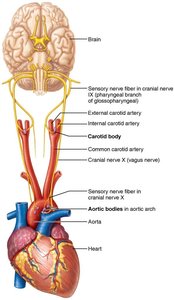
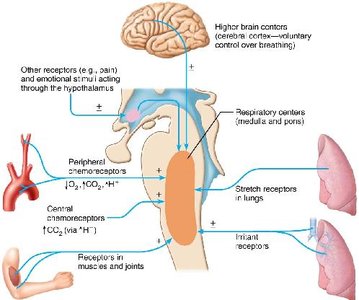
Chemical factors: Most important; include PCO2, PO2, and pH.
Higher brain centers: Hypothalamic and cortical controls.
Pulmonary irritant reflexes: Respond to irritants and promote constriction of air passages.
Inflation reflex: Hering-Breuer reflex; stretch receptors in lungs send inhibitory signals to end inhalation.
Respiratory Adjustments
Exercise
During exercise, ventilation increases to meet metabolic needs. Hyperpnea is the increased ventilation in response to exercise, and is regulated by psychological stimuli, cortical motor activation, and proprioceptor impulses. PCO2, PO2, and pH remain constant during exercise.
High Altitude
At high altitudes, lower atmospheric pressure and PO2 can cause acute mountain sickness. Acclimatization involves increased ventilation and RBC production to compensate for lower O2 availability.
Lung Diseases
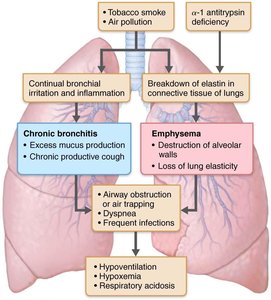
Chronic Obstructive Pulmonary Disease (COPD)
COPD is characterized by an irreversible decrease in the ability to force air out of the lungs. It includes chronic emphysema and chronic bronchitis, with symptoms such as dyspnea, coughing, frequent infections, hypoventilation, respiratory acidosis, and hypoxemia.
Emphysema: Permanent enlargement of alveoli and destruction of alveolar walls, leading to decreased lung elasticity.
Chronic bronchitis: Chronic excessive mucus production and inflammation of lower respiratory passageways.
Asthma
Asthma is characterized by acute episodes of airway inflammation, bronchospasms, coughing, dyspnea, wheezing, and chest tightness. It is an immune response involving interleukins, IgE, and inflammatory cells.
Tuberculosis (TB)
TB is an infectious disease caused by Mycobacterium tuberculosis, with symptoms including fever, night sweats, weight loss, and coughing up blood. Treatment involves a long course of antibiotics, but resistant strains are emerging.
Lung Cancer
Lung cancer is the leading cause of cancer deaths in North America, with 90% of cases due to smoking. The three most common types are adenocarcinoma, squamous cell carcinoma, and small cell carcinoma. Early detection is key to survival.
Sleep Apnea
Sleep apnea is a disorder characterized by temporary cessation of breathing during sleep, leading to excessive daytime sleepiness and increased risk of chronic illnesses. Obstructive sleep apnea is caused by collapse of the upper airway, while central sleep apnea is due to reduced drive from respiratory centers.
Cystic Fibrosis
Cystic fibrosis is the most common lethal genetic disease in North America, caused by an abnormal gene for the Cl– membrane channel protein (CFTR). It results in abnormal, viscous mucus that clogs passageways and leads to infections. Treatments include mucus-dissolving drugs, antibiotics, and ongoing research into gene therapy.
Developmental Aspects of the Respiratory System
Embryonic Development
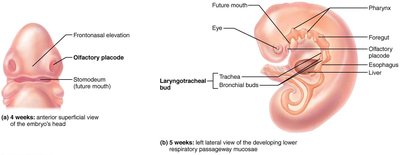
Upper respiratory structures develop first, with olfactory placodes forming nasal cavities by week 4 and the laryngotracheal bud present by week 5. By week 28, a premature baby can breathe on its own. During fetal life, lungs are filled with fluid and gas exchange occurs via the placenta.
Postnatal Development
At birth, respiratory centers are activated, alveoli inflate, and lungs begin to function. Respiratory rate is highest in newborns and decreases with age. Lungs continue to mature until young adulthood, but respiratory efficiency decreases in old age.
Factor | Effect on O2 Unloading | Curve Shift |
|---|---|---|
↑ Temperature, ↑ PCO2, ↓ pH, ↑ BPG | Increases O2 unloading | Right |
↓ Temperature, ↓ PCO2, ↑ pH, ↓ BPG | Decreases O2 unloading | Left |
Additional info: The notes above expand on brief points with academic context, definitions, and examples to ensure completeness and clarity for exam preparation.
