 Back
BackAnemia and Erythrocyte Disorders: Mechanisms, Types, and Clinical Features
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Anemia and Erythrocyte Disorders
Overview of Oxygen Transport and Erythropoiesis
Anemia and related erythrocyte disorders are conditions that affect the oxygen-carrying capacity of blood, primarily through changes in red blood cell (RBC) number, structure, or function. The regulation of erythrocyte production (erythropoiesis) is tightly controlled by feedback mechanisms involving the kidneys and bone marrow.
Oxygen Transport: Nearly all (97%) of oxygen in blood is transported bound to hemoglobin in RBCs; only 3% is dissolved in plasma.
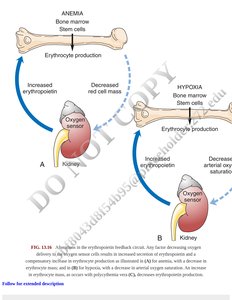
Erythropoiesis: The process by which new RBCs are produced in the bone marrow, stimulated by erythropoietin (EPO) released from the kidneys in response to hypoxia (low oxygen levels).
Feedback Regulation: Anemia or hypoxia triggers increased EPO production, stimulating the bone marrow to produce more RBCs.
Key Points in Oxygen Transport and Anemia
Hemoglobin saturation and oxygen delivery depend on partial pressure of oxygen (PO2), pH, and temperature.
CO2 is transported in blood as bicarbonate, dissolved gas, or bound to hemoglobin.
Anemia leads to decreased oxygen-carrying capacity, resulting in tissue hypoxia and compensatory mechanisms such as increased heart rate and respiratory rate.
Classification of Anemia and Polycythemia
Types of Anemia
Anemia is classified based on the underlying cause, which may include decreased RBC production, increased RBC destruction, or blood loss. Polycythemia refers to increased RBC mass.
Anemia Type | Subtypes/Examples |
|---|---|
Decreased RBC Production | Aplastic anemia, chronic renal failure, iron deficiency, vitamin B12/folate deficiency, thalassemia |
Increased RBC Destruction | Sickle cell anemia, hereditary spherocytosis, G6PD deficiency, hemolytic disease of the newborn |
Blood Loss | Acute or chronic hemorrhage |
Polycythemia | Relative (dehydration), absolute (primary/secondary polycythemia) |

General Effects and Clinical Manifestations of Anemia
Symptoms: Fatigue, pallor, shortness of breath, tachycardia, and dizziness due to reduced oxygen delivery.
Compensatory Mechanisms: Increased cardiac output, redistribution of blood flow, and increased 2,3-DPG in RBCs to enhance oxygen release.
Severity: Symptoms depend on the rate of onset, degree of anemia, and underlying cause.
Anemia Related to Decreased RBC Production
Aplastic Anemia
Aplastic anemia is characterized by failure of the bone marrow to produce adequate numbers of all blood cells, leading to pancytopenia (deficiency of RBCs, WBCs, and platelets).
Etiology: Can be caused by radiation, chemicals, drugs, infections, or idiopathic factors.
Laboratory Findings: Low RBC, WBC, and platelet counts; low reticulocyte count.
Treatment: Immunosuppressive therapy, bone marrow transplantation.
Anemia of Chronic Kidney Disease
Chronic kidney disease leads to decreased erythropoietin production, resulting in reduced RBC synthesis.
Laboratory Findings: Normocytic, normochromic anemia; low reticulocyte count.
Treatment: Erythropoiesis-stimulating agents, iron supplementation.
Anemia Due to Vitamin B12 or Folate Deficiency
Deficiency of vitamin B12 or folate impairs DNA synthesis, leading to megaloblastic anemia with large, immature RBCs.
Etiology: Poor dietary intake, malabsorption, increased requirements.
Laboratory Findings: Macrocytic anemia (high MCV), low reticulocyte count, hypersegmented neutrophils.
Treatment: Vitamin B12 or folate supplementation.
Iron Deficiency Anemia
Iron deficiency is the most common cause of anemia worldwide, resulting in microcytic, hypochromic RBCs.
Etiology: Chronic blood loss, poor dietary intake, increased requirements.
Laboratory Findings: Low MCV, low MCHC, low serum ferritin, high total iron-binding capacity (TIBC).
Treatment: Iron supplementation and treatment of underlying cause.
Anemia Related to Inherited Disorders of the Red Cell
Thalassemia
Thalassemias are inherited disorders characterized by decreased synthesis of either alpha or beta globin chains, leading to ineffective erythropoiesis and hemolysis.
Types: Alpha-thalassemia, beta-thalassemia.
Laboratory Findings: Microcytic, hypochromic anemia; target cells on blood smear.
Treatment: Regular transfusions, iron chelation therapy, bone marrow transplantation.

Sickle Cell Anemia
Sickle cell anemia is caused by a mutation in the beta-globin gene, resulting in abnormal hemoglobin S that polymerizes under low oxygen conditions, causing RBCs to become rigid and sickle-shaped.
Pathophysiology: Sickled RBCs occlude small vessels, leading to ischemia, pain, and organ damage; increased hemolysis causes anemia and jaundice.
Laboratory Findings: Sickle-shaped RBCs, increased reticulocyte count, target cells.
Treatment: Hydroxyurea, transfusions, bone marrow transplantation.

Laboratory Findings for Erythrocyte Disorders
Laboratory evaluation of anemia includes complete blood count (CBC), reticulocyte count, blood smear, and specific tests for hemolysis or nutrient deficiencies.
Disease | HCT | HB | MCV | MCH | MCHC | Retic | RBC | WBC | PLT | Blood Smear | Laboratory Tests |
|---|---|---|---|---|---|---|---|---|---|---|---|
Relative anemia | Low | Low | Normal | Normal | Normal | Low | Low | Normal | Normal | Normal | Decreased plasma volume |
Aplastic anemia | Low | Low | Normal | Normal | Normal | Low | Low | Low | Low | Normocytic, normochromic | Bone marrow biopsy |
Iron deficiency | Low | Low | Low | Low | Low | Low | Low | Normal | Normal | Microcytic, hypochromic | Serum ferritin, TIBC |
Sickle cell anemia | Low | Low | Normal | Normal | Normal | High | Low | Normal | Normal | Sickled cells | Hemoglobin electrophoresis |
Hereditary spherocytosis | Low | Low | Normal | Normal | Normal | High | Low | Normal | Normal | Spherocytes | Osmotic fragility test |
G6PD deficiency | Low | Low | Normal | Normal | Normal | High | Low | Normal | Normal | Bite cells, Heinz bodies | G6PD assay |

Inherited and Acquired Hemolytic Anemias
Hereditary Spherocytosis
Hereditary spherocytosis is caused by defects in RBC membrane proteins, leading to spherical, fragile RBCs that are prone to hemolysis.
Laboratory Findings: Spherocytes on blood smear, increased osmotic fragility.
Treatment: Splenectomy in severe cases.
Glucose-6-Phosphate Dehydrogenase (G6PD) Deficiency
G6PD deficiency is an X-linked disorder causing episodic hemolysis in response to oxidative stress (e.g., certain drugs, infections, fava beans).
Laboratory Findings: Bite cells, Heinz bodies on blood smear.
Treatment: Avoidance of triggers.
Hemolytic Disease of the Newborn (HDN)
HDN results from maternal antibodies against fetal RBC antigens, leading to hemolysis in the fetus or newborn.
Prevention: Administration of anti-Rh immunoglobulin to Rh-negative mothers.
Summary Table: Complications of Sickle Cell Anemia
Complication | Incidence | Features |
|---|---|---|
Painful crisis | 50% of patients with HbSS | Mild to severe pain, often recurrent |
Chest syndrome | Variable | Acute chest pain, fever, pulmonary infiltrates |
Priapism | Common in males | Painful, prolonged erection |
Stroke | Children and adults | Neurological deficits |
Leg ulcers | Adolescents and adults | Chronic, non-healing ulcers |

Key Points
Anemia results in tissue hypoxia and compensatory physiological responses.
Classification of anemia is based on etiology, RBC indices, and laboratory findings.
Inherited and acquired disorders can affect RBC production, structure, or survival.
Laboratory evaluation is essential for diagnosis and management.
