 Back
BackThe Urinary System: Structure, Function, and Regulation
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Urinary System: Overview and Functions
Excretion and Participating Organ Systems
The process of excretion involves removing wastes and excess materials from the body to maintain homeostasis. Several organ systems contribute to excretion:
Digestive system: Excretes food residues and wastes produced by the liver.
Respiratory system: Removes carbon dioxide via the lungs.
Integumentary system: Excretes water and salts through the skin.
Urinary system: Excretes nitrogenous wastes, excess solutes, and water via the kidneys.
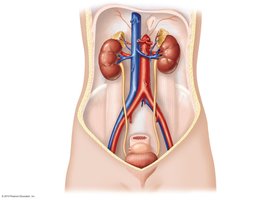
Structures of the Urinary System
The urinary system is composed of several key structures that work together to produce, transport, store, and eliminate urine:
Two kidneys: Produce urine by filtering blood.
Two ureters: Muscular tubes that transport urine from the kidneys to the bladder.
One urinary bladder: Stores urine until excretion.
One urethra: Conducts urine from the bladder to the outside of the body.
Urine is composed primarily of water and solutes. The kidneys regulate the amount of water and salt excreted, maintaining the body's fluid volume and composition. Essential nutrients such as carbohydrates, lipids, and proteins are retained and not excreted by the kidneys.
Kidney Function and Regulation
Regulation of Water and Solutes
The kidneys play a central role in regulating water levels and solute concentrations in the body:
Water input: Comes from food, drink, and metabolism.
Water output: Occurs via lungs, skin, feces, and kidneys.
The kidneys adjust water output to match intake and loss, varying from 0.5 liters/day to 1 liter/hour.
Protein metabolism produces nitrogenous wastes such as ammonia, which is converted by the liver to urea for safer transport and excretion. The kidneys also regulate other solutes, including sodium, chloride, potassium, calcium, hydrogen ions, and creatinine.
Organs and Internal Structure of the Urinary System
Kidneys: Principal organs, with an outer cortex, inner medulla, and a central renal pelvis where urine collects.
Ureters: Muscular tubes transporting urine to the bladder.
Urinary bladder: Stores 600–1000 ml of urine, lined with epithelial cells and smooth muscle.
Urethra: Conducts urine out of the body, controlled by internal (smooth muscle) and external (skeletal muscle) sphincters.
The Nephron: Functional Unit of the Kidney
Each kidney contains about one million nephrons, which are responsible for filtering blood and forming urine. Each nephron consists of:
Tubule: A thin, hollow tube of epithelial cells.
Associated blood supply: Includes specialized capillaries.
Nephrons remove approximately 180 liters of fluid from the blood daily, returning most to the bloodstream minus the wastes to be excreted.
Nephron Structure
Glomerular capsule (Bowman's capsule): Surrounds the glomerulus, where filtration occurs.
Proximal tubule: Extends from the capsule into the medulla.
Loop of Henle: Dips into the medulla and returns to the cortex.
Distal tubule: Further modifies filtrate.
Collecting duct: Shared by several nephrons, empties into the renal pelvis.
Blood Supply to the Nephron
Renal artery: Supplies blood to the kidney.
Afferent arteriole: Brings blood to the glomerulus.
Efferent arteriole: Carries blood away from the glomerulus.
Glomerular capillaries: Site of filtration.
Peritubular capillaries: Surround the proximal and distal tubules.
Vasa recta: Parallels the loop of Henle.
Renal vein: Returns filtered blood to circulation.
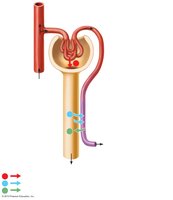
Urine Formation: Filtration, Reabsorption, and Secretion
Three Major Renal Processes
Urine formation involves three key processes:
Glomerular filtration: Protein-free fluid and solutes move from blood into the glomerular capsule.
Tubular reabsorption: Most filtered water and solutes are returned to the blood.
Tubular secretion: Additional solutes are secreted from blood into the tubule.
Glomerular Filtration
Filters large volumes of protein-free plasma from capillaries into the glomerular capsule.
Highly selective—impermeable to large proteins and cells.
Driven by high blood pressure in glomerular capillaries.
Filtration rate is regulated by local control (arteriole diameter) and the sympathetic nervous system (during stress).
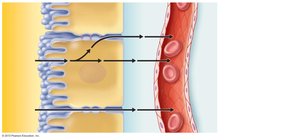
Tubular Reabsorption
Returns 100% of filtered glucose, amino acids, and bicarbonate, and about 50% of urea to the blood.
Most reabsorption occurs in the proximal tubule (65–70% of water), with additional reabsorption in the loop of Henle (25%) and distal tubule/collecting duct (<10%).
Brush border microvilli on proximal tubule cells increase surface area for reabsorption.
Tubular Secretion
Moves substances from blood (peritubular capillaries or vasa recta) into the tubule for excretion.
Regulates chemical levels and removes harmful substances (e.g., drugs, hydrogen ions, potassium).
Regulation of Urine Concentration
Producing Dilute Urine
When excess water is present, kidneys reabsorb less water, producing dilute urine.
Distal tubule is impermeable to water; NaCl is reabsorbed without water, resulting in high-volume, dilute urine.
Producing Concentrated Urine
When water is scarce, kidneys conserve water by producing concentrated urine.
Mediated by antidiuretic hormone (ADH) from the posterior pituitary, which increases collecting duct permeability to water, enhancing reabsorption.
Control of Urination (Micturition)
Micturition reflex: Neural reflex triggered by stretch receptors in the bladder wall.
Internal urethral sphincter (smooth muscle) and external urethral sphincter (skeletal muscle, voluntary control) regulate urination.
The brain can override the reflex, but voluntary control decreases as the bladder fills.
Homeostatic Functions of the Kidneys
Maintain water and salt balance.
Secrete enzymes for blood volume and pressure control.
Regulate acid-base balance and blood pH.
Stimulate red blood cell production via erythropoietin.
Activate vitamin D.
Hormonal Regulation: Antidiuretic Hormone (ADH)
ADH and Water Balance
Blood volume and pressure are tightly regulated by ADH.
Hypothalamus: Synthesizes ADH.
Posterior pituitary: Releases ADH.
Kidneys: Respond to ADH by adjusting water reabsorption.
Negative feedback loop adjusts ADH secretion and thirst to maintain solute concentration.
Effects of ADH
If blood solute concentration is high (low water), ADH is released, increasing water reabsorption and decreasing urine output.
If blood solute concentration is low (high water), ADH secretion decreases, reducing water reabsorption and increasing urine output.
Diuresis and Diuretics
Diuresis: High urine flow rate.
Diuretics: Substances that increase urine formation (e.g., Lasix, caffeine, alcohol).
Lasix inhibits sodium reabsorption; caffeine inhibits sodium reabsorption; alcohol inhibits ADH release.
Disorders of the Urinary System
Kidney Stones
Crystallized minerals that may block urine flow in ureters.
Treatment: Ultrasound or surgical removal.
Urinary Tract Infections (UTIs)
Usually caused by bacteria (often E. coli), more common in women.
Symptoms: Pelvic pain, pain/burning during urination, back pain, blood in urine.
Treatment: Antibiotics.
Acute Renal Failure
Short-term impairment, potentially reversible.
Causes: Low blood pressure, kidney stones, infections, injury, toxins, drug reactions.
Chronic Renal Failure (End-Stage Renal Disease, ESRD)
Long-term, irreversible loss of kidney function (>60% reduction in nephrons).
Often caused by diabetes (diabetic nephropathy).
Patients may require dialysis or kidney transplant.
Dialysis
CAPD (Continuous Ambulatory Peritoneal Dialysis): Uses peritoneal cavity for waste exchange; risk of infection.
Hemodialysis: Blood is filtered through a machine; requires regular visits to a dialysis center.
Dialysis does not fully replicate kidney function; hormone supplementation (e.g., erythropoietin) may be needed.
Kidney Transplants
Permanent solution for ESRD.
Success improved by better tissue matching and anti-rejection medications.
Organ shortage remains a challenge.
Urinary Incontinence
Loss of bladder control, more common with age and in women.
Causes: Aging, pregnancy, childbirth, menopause, prostate issues in men.
Treatments: Bladder training, exercises, fluid management, medications, surgery.
