 Back
BackThe Urinary System: Structure, Function, and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Urinary System
Overview and Major Functions
The urinary system is essential for maintaining the body's internal environment by regulating water, solute concentrations, and removing metabolic wastes. It also plays important endocrine and metabolic roles.
Regulation of water and solute balance: Maintains total water volume and solute concentration in the body.
Ion regulation: Controls extracellular fluid (ECF) ion concentrations.
Acid-base balance: Ensures long-term acid-base equilibrium.
Excretion: Removes metabolic wastes, toxins, and drugs from the body.
Endocrine functions: Secretes renin (regulates blood pressure), erythropoietin (stimulates red blood cell production), and activates vitamin D.
Gluconeogenesis: Generates glucose during prolonged fasting.
Organs of the Urinary System
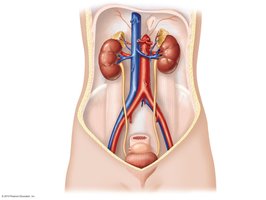
The urinary system consists of the kidneys, ureters, urinary bladder, and urethra, each with specialized roles in urine formation and excretion.
Kidneys: Major excretory organs; filter blood and form urine.
Ureters: Transport urine from kidneys to the urinary bladder.
Urinary bladder: Temporary storage reservoir for urine.
Urethra: Transports urine out of the body.
Anatomy of the Kidneys
Location and Structure
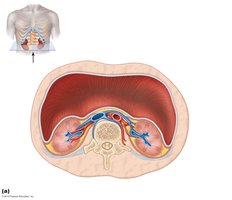
The kidneys are retroperitoneal organs located against the posterior body wall, protected by the lower ribs and surrounded by supportive tissue layers.
Position: Lie between the T12 and L3 vertebrae, partially protected by the 12th rib.
Supportive tissues: Include the renal fascia, perirenal fat capsule, and fibrous capsule.

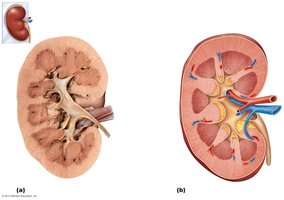
Internal Anatomy
The kidney is divided into the renal cortex, renal medulla, and renal pelvis. The cortex contains the majority of nephrons, while the medulla is organized into pyramids. The renal pelvis collects urine before it enters the ureter.
Renal cortex: Outer region containing renal corpuscles and convoluted tubules.
Renal medulla: Inner region with renal pyramids and columns.
Renal pelvis: Funnel-shaped structure that collects urine from major and minor calyces.
Homeostatic Imbalances
Pyelitis: Infection of the renal pelvis and calyces.
Pyelonephritis: Infection/inflammation of the entire kidney, usually treatable with antibiotics.
Nephrons: The Functional Units of the Kidney
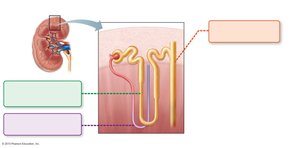
Structure of the Nephron
Each kidney contains about one million nephrons, which filter blood and form urine. The nephron consists of the renal corpuscle and renal tubule.
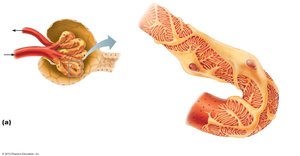
Renal corpuscle: Includes the glomerulus (a tuft of capillaries) and glomerular (Bowman's) capsule (surrounds the glomerulus).
Renal tubule: Composed of the proximal convoluted tubule (PCT), nephron loop (loop of Henle), distal convoluted tubule (DCT), and collecting duct.

Classes of Nephrons
Cortical nephrons: 85% of nephrons; located almost entirely in the cortex.
Juxtamedullary nephrons: Long nephron loops extend deep into the medulla; essential for producing concentrated urine.
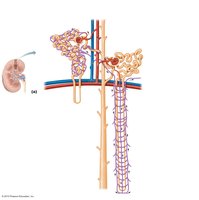
Nephron Capillary Beds
Peritubular capillaries: Low-pressure, porous capillaries adapted for absorption; surround cortical nephrons.
Vasa recta: Long, straight capillaries paralleling nephron loops of juxtamedullary nephrons; crucial for urine concentration.
Mechanisms of Urine Formation
Overview of Renal Processes
The kidneys process about 180 liters of fluid daily, but only 1.5 liters become urine. Three main processes adjust blood composition:
Glomerular filtration: Passive process producing cell- and protein-free filtrate.
Tubular reabsorption: Selectively returns 99% of substances from filtrate to blood.
Tubular secretion: Selectively moves substances from blood to filtrate.
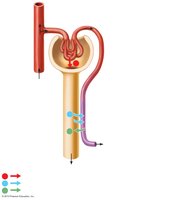
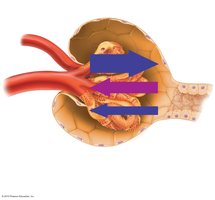
Glomerular Filtration
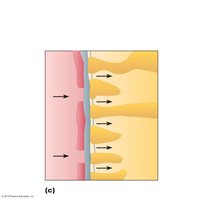
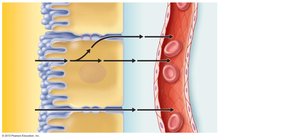
Filtration occurs across a specialized membrane in the renal corpuscle, driven by hydrostatic pressure. The filtration membrane consists of three layers: capillary endothelium, basement membrane, and podocyte foot processes.
Filtration membrane: Allows passage of water and small solutes; blocks blood cells and proteins.
Net filtration pressure (NFP): Determined by the balance of hydrostatic and osmotic pressures.
Equation for NFP:
Where:
HPgc = Glomerular capillary hydrostatic pressure (55 mm Hg)
HPcs = Capsular hydrostatic pressure (15 mm Hg)
OPgc = Glomerular capillary colloid osmotic pressure (30 mm Hg)
Example calculation: mm Hg
Glomerular Filtration Rate (GFR)
Normal GFR: 120–125 ml/min for both kidneys.
Factors affecting GFR: Net filtration pressure, surface area, and membrane permeability.
Tubular Reabsorption
Most filtrate is reabsorbed into the blood via active and passive processes. Reabsorption can occur through transcellular (across cells) or paracellular (between cells) routes.
All organic nutrients (e.g., glucose, amino acids) are reabsorbed.
Water and ion reabsorption is hormonally regulated.
Transport Maximum (Tm)
Each substance has a maximum rate of reabsorption, determined by the number of transport proteins.
Excess substances (e.g., glucose in diabetes) are excreted in urine when Tm is exceeded.
Reabsorptive Capabilities of Renal Tubules and Collecting Ducts
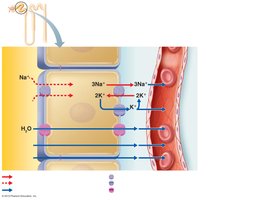
PCT: Site of most reabsorption (all nutrients, 65% Na+ and water, many ions).
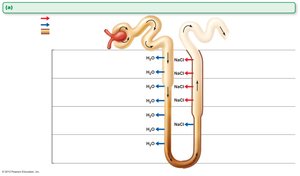
Nephron loop: Descending limb permeable to water, ascending limb permeable to solutes (Na+, Cl-).
Tubular Secretion
Secretion removes additional wastes from the blood, regulates potassium, and helps control blood pH by secreting H+ or HCO3-.
Disposes of drugs, toxins, and excess ions.
Occurs mainly in the PCT.

Regulation of Urine Concentration and Volume
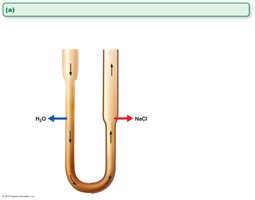
Osmolality and Countercurrent Mechanism
The kidneys maintain plasma osmolality (~300 mOsm) by regulating urine concentration and volume using a countercurrent mechanism. This mechanism establishes an osmotic gradient from cortex to medulla, allowing the kidneys to produce urine of varying concentration.
Osmolality: Number of solute particles per kilogram of water (mOsm).
Countercurrent multiplier: Long nephron loops create the gradient.
Countercurrent exchanger: Vasa recta preserve the gradient.
Collecting ducts: Use the gradient to adjust urine osmolality under hormonal control (ADH).

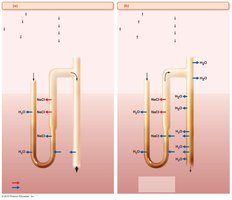
Hormonal Regulation and Urine Concentration
Antidiuretic hormone (ADH) controls water reabsorption in the collecting ducts. Overhydration suppresses ADH, producing dilute urine; dehydration increases ADH, producing concentrated urine. Urea recycling also contributes to the medullary osmotic gradient.
Diuretics
ADH inhibitors: e.g., alcohol, increase urine output.
Na+ reabsorption inhibitors: e.g., caffeine, certain drugs.
Loop diuretics: Inhibit medullary gradient formation.
Osmotic diuretics: Substances not reabsorbed, e.g., glucose in diabetes, keep water in urine.
Homeostatic Imbalances
Chronic renal disease: GFR < 60 ml/min for 3 months (e.g., diabetes, hypertension).
Renal failure: GFR < 15 ml/min; leads to uremia, treated with dialysis or transplant.
Physical and Chemical Characteristics of Urine
Physical Characteristics
Color and transparency: Clear, pale to deep yellow (urochrome pigment); abnormal colors may indicate pathology or diet.
Odor: Slightly aromatic when fresh; ammonia odor develops upon standing; certain foods and drugs can alter odor.
pH: Slightly acidic (~pH 6); varies with diet and health.
Specific gravity: 1.001 to 1.035, depending on solute concentration.
Chemical Composition
Water: 95% of urine volume.
Solutes: 5%, including nitrogenous wastes (urea, uric acid, creatinine) and ions (Na+, K+, PO43-, SO42-, Ca2+, Mg2+, HCO3-).
Abnormal components: High concentrations of normal constituents or presence of blood proteins, WBCs, or bile pigments may indicate disease.
