 Back
BackAchieving and Maintaining a Healthful Body Weight
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Achieving and Maintaining a Healthful Body Weight
What Is a Healthful Body Weight?
A healthful body weight is one that is appropriate for an individual's age and physical development, is achievable and sustainable without constant dieting, and is compatible with normal blood pressure, lipid levels, and glucose tolerance. It should be based on genetic background and family history, supported by good eating habits, allow for regular physical activity, and be personally acceptable.
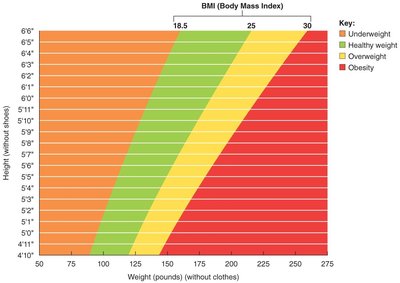
Underweight: BMI less than 18.5 kg/m2; too little body fat to maintain health.
Normal weight: BMI between 18.5 and 24.9 kg/m2.
Overweight: BMI between 25 and 29.9 kg/m2; moderate excess body fat.
Obese: BMI between 30 and 39.9 kg/m2; excess body fat that increases disease risk.
Morbid obesity: BMI ≥ 40 kg/m2; body weight exceeding 100% of normal, very high risk for health consequences.
Evaluating Body Weight
To determine if a person's body weight is healthful, three main assessments are used: Body Mass Index (BMI), body composition, and fat distribution pattern.
BMI: Ratio of weight to height squared. Calculated as:
Limitations of BMI: Does not indicate body composition, not suitable for older adults, children, athletes, pregnant or lactating women, and does not account for ethnic differences.
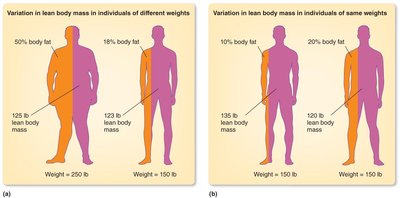
Body Composition
Body composition refers to the proportion of fat and lean tissue in the body. Several methods are used to estimate body composition, each with its own advantages and limitations.
Method | Advantages | Limitations |
|---|---|---|
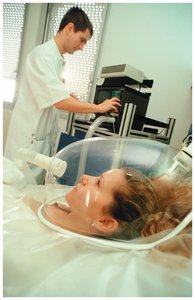
Underwater weighing | Accurate, gold standard | Uncomfortable, not suitable for all |
Skinfolds | Inexpensive, portable | Technician skill required, less accurate in obese |
Bioelectric impedance analysis (BIA) | Quick, easy | Accuracy affected by hydration status |
Dual-energy x-ray absorptiometry (DXA) | Very accurate | Expensive, requires trained personnel |
Bod Pod | Accurate, quick | Expensive, limited availability |

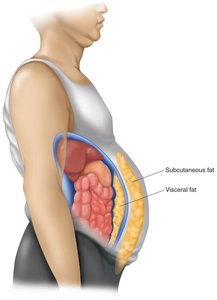
Fat Distribution Patterns
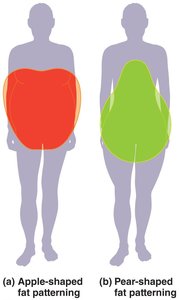
Fat distribution is an important factor in health risk. Two main patterns are recognized:
Apple-shaped (android): Fat stored in the upper body/abdomen; higher risk for chronic diseases; more common in men.
Pear-shaped (gynoid): Fat stored in the lower body (hips, thighs); not associated with increased chronic disease risk; more common in women.
Waist-to-hip ratio: Men > 0.90, Women > 0.80 indicate increased risk.
Waist circumference: Men > 40 in (102 cm), Women > 35 in (88 cm) indicate increased risk.
Energy Balance and Body Weight Regulation
Energy Balance
Energy balance is the relationship between energy intake (from food and beverages) and energy expenditure (used by the body for basic functions and physical activity). Body weight is stable when energy intake equals energy expenditure.
Energy deficit: Intake < expenditure; leads to weight loss.
Energy balance: Intake = expenditure; weight maintenance.
Energy excess: Intake > expenditure; leads to weight gain.

Energy Intake
Energy in food is measured in kilocalories (kcal). Macronutrient energy values:
Carbohydrate: 4 kcal/g
Protein: 4 kcal/g
Fat: 9 kcal/g
Alcohol: 7 kcal/g
Example: 1 cup oatmeal (6g protein, 25g carbohydrate, 2g fat): 6 × 4 + 25 × 4 + 2 × 9 = 24 + 100 + 18 = 142 kcal
Energy Expenditure
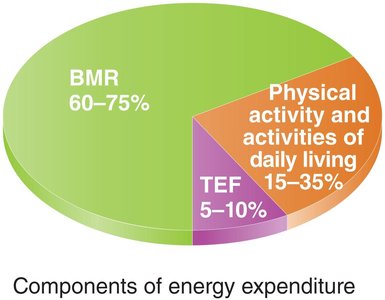
Total energy expenditure is the sum of:
Basal metabolic rate (BMR): Energy for basic body functions at rest (60–75% of total).
Thermic effect of food (TEF): Energy to digest, absorb, and metabolize food (5–10%).
Physical activity: Energy for movement and exercise (15–35%).
Measuring Energy Expenditure
Two main methods are used:
Direct calorimetry: Measures heat released by the body.
Indirect calorimetry: Estimates energy expenditure by measuring oxygen consumption and carbon dioxide production.
Basal Metabolic Rate (BMR)
BMR is the energy expended to maintain basic physiological functions such as respiration, circulation, and cell synthesis. The primary determinant is lean body mass.
BMR varies widely among individuals.
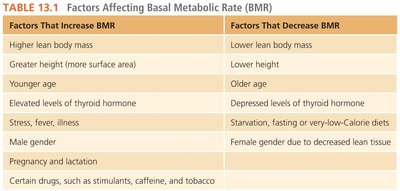
Factors affecting BMR include age, gender, body composition, thyroid hormone levels, and more.
Factors That Increase BMR | Factors That Decrease BMR |
|---|---|
Higher lean body mass | Lower lean body mass |
Greater height | Lower height |
Younger age | Older age |
Elevated thyroid hormone | Depressed thyroid hormone |
Stress, fever, illness | Starvation, very-low-calorie diets |
Male gender | Female gender (less lean tissue) |
Pregnancy, lactation | |
Certain drugs (stimulants, caffeine, tobacco) |
Physical Activity and Energy Expenditure
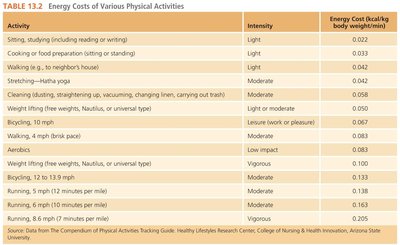
Physical activity significantly increases total energy expenditure. The energy cost depends on the type, intensity, and duration of activity.
Activity | Intensity | Energy Cost (kcal/kg body weight/min) |
|---|---|---|
Sitting, studying | Light | 0.022 |
Walking (2 mph) | Light | 0.034 |
Stretching, Hatha yoga | Moderate | 0.042 |
Bicycling (10 mph) | Moderate | 0.083 |
Running (6 mph) | Vigorous | 0.165 |
Genetic, Physiological, and Environmental Factors Affecting Body Weight
Genetic Factors
Genetics play a significant role in determining body weight, shape, and metabolic rate. BMI is influenced by both genetic (50–90%) and environmental/lifestyle factors (10–90%). Key genetic theories include:
FTO gene: Associated with increased food intake and reduced satiety; physical activity can reduce its impact.
Thrifty gene theory: Suggests some people are genetically predisposed to be more energy-efficient, protecting against starvation.
Set-point theory: Proposes body weight is regulated at a predetermined, or 'set', point by physiological mechanisms.
Metabolic and Physiological Factors
Several metabolic and physiological factors influence body weight:
Low metabolic rate
Low spontaneous physical activity
Low sympathetic nervous system activity
Low fat oxidation
Abnormal thyroid hormone levels
Certain medications
Hormones and proteins also regulate appetite and energy balance:
Leptin: Produced by adipose tissue; reduces food intake.
Ghrelin: Produced in the stomach; stimulates appetite.
Peptide YY (PYY): Produced in the GI tract; decreases appetite.
Uncoupling proteins: Increase energy expenditure in brown adipose tissue.
Cultural, Economic, and Social Factors
Body weight is also influenced by cultural, economic, and social factors, including:
Religious beliefs and learned food preferences
Fast-food culture and sedentary lifestyle
Economic status and educational attainment
Access to healthcare
Psychological factors such as appetite, meal timing, mood, and social pressures
Obesity, Health Risks, and Treatment
Obesity and Morbid Obesity
Obesity (BMI 30–39.9 kg/m2) and morbid obesity (>100% normal weight or BMI ≥ 40 kg/m2) are considered epidemics in the United States and are linked to many chronic diseases, including hypertension, dyslipidemia, diabetes, heart disease, and stroke.
Metabolic Syndrome
Metabolic syndrome is a cluster of risk factors that increase the risk for heart disease, type 2 diabetes, and stroke. Criteria include abdominal obesity, high triglycerides, low HDL cholesterol, high blood pressure, and elevated fasting glucose.
Obesity as a Multifactorial Disease
Obesity results from the interaction of biological, psychological, environmental, and societal factors, including food environment and consumption, physical activity, and individual psychology.
Treatment of Obesity
Diet and Exercise: Create a 500–1000 kcal/day deficit, increase physical activity, and seek counseling/support.
Medications: May suppress appetite or increase satiety; require physician supervision due to potential side effects.
Supplements: Often unregulated and potentially dangerous; insufficient evidence for effectiveness.
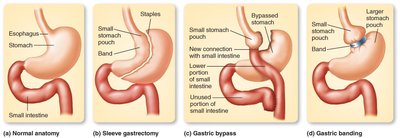
Bariatric Surgery: Last resort for morbid obesity; includes procedures such as vertical banded gastroplasty, gastric bypass, and gastric banding.
Weight-Loss Diets
High-carbohydrate, moderate fat and protein diets: Balanced, gradual weight loss (e.g., Weight Watchers, DASH diet).
Low-carbohydrate, high fat and protein diets: Promote ketosis; concerns about long-term safety (e.g., Atkins, Paleo).
Low-fat and very-low-fat diets: Emphasize complex carbohydrates and fiber; lower LDL cholesterol and blood pressure (e.g., Ornish, Pritikin).
Strategies for Achieving and Maintaining a Healthful Weight
Set specific, reasonable, and measurable goals.
Follow recommended serving sizes and reduce high-fat, high-energy foods.
Choose foods low in energy density.
Engage in regular physical activity.
Incorporate behavior modifications into daily life.
Underweight and Safe Weight Gain
Risks of Being Underweight
Being underweight (BMI < 18.5 kg/m2) can be as harmful as obesity and may result from genetics, insufficient caloric intake, heavy smoking, underlying disease, or eating disorders such as anorexia nervosa.
Safe and Effective Weight Gain
Limit fat intake to <30% of total energy.
Increase caloric intake by 500–1,000 kcal/day.
Eat frequently throughout the day.
Avoid tobacco (suppresses appetite, increases BMR).
Engage in resistance training to build lean mass.
Protein Supplements
Protein and amino acid supplements, anabolic steroids, and androstenedione do not enhance muscle gain or strength and may cause serious health problems, including unhealthful changes in blood cholesterol and mood disturbances.
