 Back
BackDisorders of Swallowing: Evaluation and Management
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Disorders of Swallowing (Dysphagia)
Introduction to Swallowing and Dysphagia
Swallowing is a complex process essential for nutrition and hydration. Dysphagia refers to difficulty with eating or swallowing and can affect individuals across the lifespan. Speech-language pathologists (SLPs) play a central role in the evaluation and management of dysphagia in both pediatric and adult populations. Dysphagia can lead to medical complications such as malnutrition, dehydration, aspiration pneumonia, and psychosocial issues including isolation and reduced quality of life.
Normal and Disordered Swallowing
Phases of Normal Swallowing
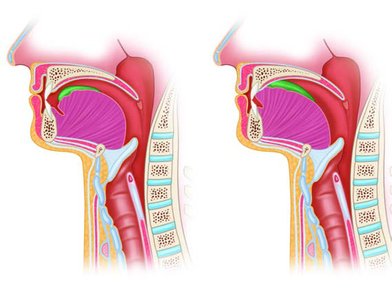
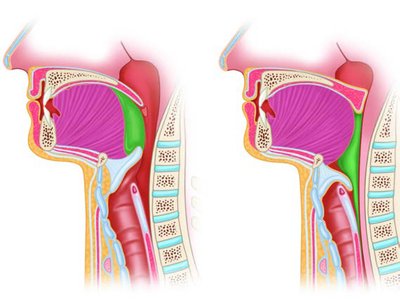
Swallowing is divided into four main phases, each with distinct anatomical and physiological features:
Oral Preparation Phase: Food is chewed and mixed with saliva to form a bolus. The tongue and cheeks help position the bolus for swallowing.
Oral Transport Phase: The tongue propels the bolus from the front to the back of the mouth, triggering the pharyngeal swallow reflex.
Pharyngeal Phase: The velum elevates to close off the nasal cavity, the larynx elevates and closes to protect the airway, and the pharyngeal muscles contract to move the bolus toward the esophagus.
Esophageal Phase: Peristaltic contractions move the bolus through the esophagus into the stomach.
Disordered Swallowing (Dysphagia)
Dysphagia can occur in any phase of swallowing and may result from structural, neurological, or functional impairments. Common problems include:
Oral Phase: Poor lip seal (drooling), impaired chewing, insufficient saliva, and poor tongue control.
Pharyngeal Phase: Delayed or absent swallow reflex, aspiration (entry of material into the airway), nasal regurgitation, and pharyngeal residue.
Esophageal Phase: Impaired peristalsis, esophageal residue, and reflux.

Etiologies of Pediatric and Adult Dysphagia
Common Causes in Children
Prematurity: Immature suck-swallow-breathe coordination, often requiring tube feeding.
Cerebral Palsy: Poor oral motor control, reflux, and need for gastrostomy tube in severe cases.
Intellectual and Developmental Disabilities: Delayed motor skills and communication barriers.
Autism Spectrum Disorder: Sensory aversions and restricted diets leading to poor nutrition.
Craniofacial Anomalies: Cleft lip/palate causing feeding and swallowing difficulties.

Common Causes in Adults
Stroke: Oral-motor and sensory deficits, poor bolus control, and risk of silent aspiration.
Head and Neck Cancer: Surgery and radiation affecting swallowing structures and function.
Parkinson Disease: Reduced coordination, delayed swallow, and esophageal dysmotility.
Traumatic Brain Injury: Motor and cognitive deficits affecting safe swallowing.
Dementia: Impaired attention, memory, and oral motor function.
Evaluation for Swallowing Disorders
Screening for Dysphagia
Screening identifies individuals at risk for dysphagia. For adults, tools like the Yale Swallow Protocol (YSP) are used, involving cognitive screening, oral mechanism examination, and a water swallow test. For infants and children, feeding observations and growth monitoring are key.

Clinical Swallow Evaluation (CSE)
The CSE includes:
Case history and background information
Cognitive-communication assessment
Observation of environmental and caregiver factors
Oral mechanism examination (lips, tongue, palate, cranial nerves)
Swallow trials with various food and liquid consistencies
Instrumental Swallow Examination
Videofluoroscopic Swallowing Study (VFSS/MBSS): X-ray procedure using barium to visualize swallowing function and detect aspiration or residue.
Fiberoptic Endoscopic Evaluation of Swallowing (FEES): Flexible scope inserted through the nose to directly observe pharyngeal and laryngeal structures during swallowing.



Treatment of Swallowing Disorders
Compensatory Strategies
Modify feeding environment (reduce distractions, appropriate lighting, attentive caregivers)
Use of specialized feeding utensils (e.g., slow-flow nipples, shallow-bowled spoons, cutout cups)
Diet modification (altering food texture and liquid viscosity according to the International Dysphagia Diet Standardization Initiative, IDDSI)
Nonoral feeding methods (NG tube, PEG/G-tube, J-tube, total parenteral nutrition)
Body and head positioning (upright posture, chin tuck, head rotation)




Direct and Indirect Rehabilitative Treatments
Exercise-Based Therapy: Strengthening and coordination exercises for swallowing muscles (e.g., tongue resistance training, effortful swallow, Mendelsohn maneuver).
Swallowing-Specific Exercises: Effortful swallow, supraglottic and super-supraglottic swallow, Mendelsohn maneuver.
Surface Electromyography (sEMG): Biofeedback tool for muscle activation during swallowing exercises.
Neuromuscular Electrical Stimulation (NMES): Electrical stimulation to enhance muscle contraction and swallowing function.


Prostheses and Surgical Procedures
Palatal obturators for soft palate defects
Tongue prostheses for glossectomy patients
Additional SLP strategies to optimize prosthetic use
Summary Table: Common Etiologies of Feeding and Swallowing Disorders
Population | Etiology | Description |
|---|---|---|
Children | Prematurity | Immature suck-swallow-breathe coordination, tube feeding often required |
Children | Cerebral Palsy | Poor oral motor control, reflux, possible need for gastrostomy tube |
Children | ASD | Sensory aversions, restricted diets, risk of poor nutrition |
Adults | Stroke | Oral-motor and sensory deficits, risk of aspiration |
Adults | Head and Neck Cancer | Surgical/radiation effects on swallowing structures |
Adults | Parkinson Disease | Reduced coordination, delayed swallow, esophageal dysmotility |
Key Terms
Dysphagia: Difficulty swallowing
Aspiration: Entry of food or liquid into the airway
Bolus: A mass of food or liquid prepared for swallowing
Peristalsis: Rhythmic contractions moving food through the esophagus
Videofluoroscopy: X-ray imaging of swallowing
FEES: Endoscopic visualization of swallowing
Compensatory strategies: Techniques to maintain safety and nutrition without changing swallowing physiology
Direct/Indirect rehabilitation: Exercises to improve swallowing function
