 Back
BackEating Disorders: Identification, Characteristics, and Management
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Eating Disorders: Overview
Definition and General Features
Eating disorders are serious mental illnesses characterized by abnormal or disturbed eating habits, often associated with extreme emotions, attitudes, and behaviors surrounding weight and food. These disorders can lead to significant physical and psychological health consequences and are treatable with early intervention.
Key Features: Food restriction, binge eating, purging, and weight fluctuations.
Associated Changes: Emotional and cognitive changes affecting body perception and experience.
Prevalence: Can affect all ages, genders, races, and socioeconomic groups, but are more common in adolescence and early adulthood.
Comorbidities: Often co-occur with depression, anxiety, and substance abuse.

Types of Eating Disorders
Major Diagnoses and Comparison
The three most common eating disorders are Anorexia Nervosa (AN), Bulimia Nervosa (BN), and Binge-Eating Disorder (BED). Each has distinct behavioral and physical characteristics, but all can have severe health consequences.
Feature | Anorexia Nervosa (AN) | Bulimia Nervosa (BN) | Binge-Eating Disorder (BED) |
|---|---|---|---|
Primary Behavior | Extreme restriction of food intake | Binge eating + compensatory behaviors (purging, fasting, exercise) | Binge eating without regular compensatory behaviors |
Weight | Significantly low weight | Usually normal or overweight | Often overweight or obese |
Fear of Gaining Weight | Intense, pathologically high | Intense, pathologically high | Generally absent, but body image concerns may exist |
Binge Episodes | Can occur (in binge/purge subtype) | Required for diagnosis | Required for diagnosis |
Purging | May occur | Frequent | Rare/Absent |
Mortality Risk | Highest among psychiatric disorders | Lower than AN, but higher than general population | Significant, mainly due to metabolic comorbidities |

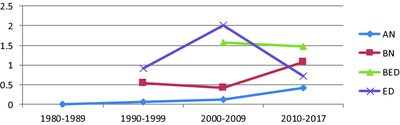
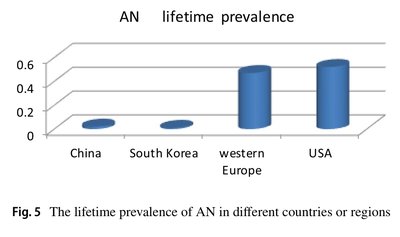
Prevalence and Trends
Recent studies show varying prevalence rates of eating disorders globally, with notable increases in certain regions and populations. For example, Bulimia Nervosa is most prevalent in Lebanon, followed by Anorexia Nervosa and Binge Eating Disorder.
Typical Profile: Single female young adult, middle to high socioeconomic status, severe symptoms.
Common Symptoms: Amenorrhea, multiple purging behaviors, depression.
Risk Factors and Etiology
Genetic, Psychological, and Social Contributors
Eating disorders are multifactorial, with genetic, psychological, and social factors all playing significant roles in their development.
Genetic: Family history of eating disorders or mental health conditions increases risk.
Psychological: Low self-esteem, perfectionism, obsessive tendencies, difficulty coping with stress or change.
Social/Cultural: Societal pressure for thinness, weight-based teasing, media influence, and certain professions (e.g., athletes, dancers, models).
Other: History of dieting, anxiety disorders, trauma, abuse, loneliness, and isolation.
Anorexia Nervosa (AN)
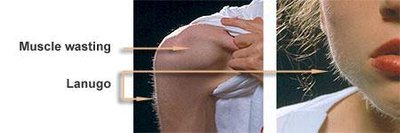
Characteristics and Warning Signs
Anorexia Nervosa is marked by self-imposed starvation and an intense fear of gaining weight, often accompanied by a distorted body image. It has the highest mortality rate among psychiatric disorders.
Behavioral Signs: Dramatic weight loss, refusal to eat certain foods, denial of hunger, excessive exercise, withdrawal from social life.
Physical Signs: Nutritional deficiencies, feeling cold, dry/scaly skin, hair loss, constipation, lanugo (fine hair growth), loss of menstrual periods, bone loss, depression.
Mortality: Up to 10% of cases may result in death, often from heart failure or suicide.
Gender: 25% of cases are male, often diagnosed later due to stereotypes.

Bulimia Nervosa (BN)
Characteristics and Diagnosis
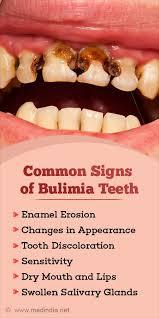
Bulimia Nervosa involves recurrent episodes of binge eating followed by compensatory behaviors such as vomiting, laxative use, or excessive exercise. Individuals often maintain a normal or above-normal weight and recognize their behavior as abnormal.
Diagnosis: Binge and purge at least once per week for three months.
Binge Triggers: Stress, boredom, loneliness, excessive dieting.
Physical Signs: Tooth decay, swollen salivary glands, blood potassium drop, stomach ulcers, callused knuckles, bloodshot eyes.
Cycle: Binge eating leads to guilt, which triggers purging and perpetuates the cycle.


Binge-Eating Disorder (BED)
Characteristics and Warning Signs
Binge-Eating Disorder is characterized by recurrent episodes of eating large quantities of food, often rapidly and to the point of discomfort, without regular compensatory behaviors. It is associated with feelings of loss of control, shame, and distress.
Warning Signs: Eating large amounts in short periods, eating alone, rapid eating, weight fluctuations, history of depression.
Physical Consequences: Increased risk of obesity, metabolic syndrome, and related health issues.

Other Specified Feeding and Eating Disorders (OSFED)
Definition and Examples
OSFED includes eating disorders that do not meet the full criteria for AN, BN, or BED but still cause significant distress or impairment. Examples include chronic dieting, orthorexia, bigorexia, night eating syndrome, and pica.
Orthorexia Nervosa: Pathological obsession with "pure" foods, leading to nutritional imbalances and social/occupational impairment.
Pica: Consumption of non-nutritive substances (e.g., clay, chalk, hair).
Treatment and Prevention
Approaches to Management
Treatment of eating disorders is multidisciplinary, involving psychological, nutritional, and medical interventions. Early intervention improves outcomes.
Psychotherapy: Individual, family therapy, cognitive-behavioral therapy (CBT).
Support Groups: Sharing experiences and support.
Nutritional Support: Education, goal setting, restoring hunger/satiety cues, supplementation.
Medication: Antidepressants and other medications as needed.
Hospitalization: For severe physical or behavioral complications.
Prevention Strategies
Creating awareness through education and advocacy.
Promoting healthy attitudes toward food, body image, and physical activity.
Encouraging early help-seeking without stigma.
Summary Table: Key Differences Between AN, BN, and BED
Disorder | Core Feature | Body Weight | Compensatory Behaviors | Psychological Features |
|---|---|---|---|---|
Anorexia Nervosa | Restriction of intake | Low | May be present (binge/purge subtype) | Intense fear of weight gain, distorted body image |
Bulimia Nervosa | Binge + purge | Normal/overweight | Frequent | Body dissatisfaction, guilt, shame |
Binge-Eating Disorder | Binge eating only | Normal to obese | Absent | Loss of control, distress, shame |
References
Wardlaw's Contemporary Nutrition: A Functional Approach (5th ed.)
National Eating Disorders Association
DSM V: Diagnostic and Statistical Manual of Mental Disorders
Relevant peer-reviewed articles and public health resources
