 Back
BackInfectious Diseases Affecting the Respiratory System: Microbiology Fundamentals
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Overview of the Respiratory System
Anatomy of the Respiratory Tract
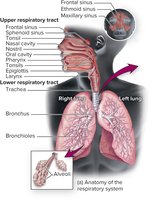
The respiratory tract is divided into the upper and lower regions, each with distinct anatomical structures and functions. Understanding these divisions is essential for recognizing how infectious diseases affect respiratory health.
Upper respiratory tract: Includes the mouth, nose, nasal cavity, sinuses, throat (pharynx), epiglottis, and larynx.
Lower respiratory tract: Comprises the trachea, bronchi, bronchioles, and alveoli.
Defenses of the Respiratory Tract
Physical and Immune Barriers
The respiratory tract is equipped with multiple defense mechanisms to prevent infection by pathogens. These defenses are both anatomical and immunological.
Nasal hair: Traps large particles and pathogens.
Cilia: Propel trapped particles upward and out of the tract.
Mucus: Acts as a sticky barrier to trap microorganisms.
Immune defenses: Include complement proteins, antimicrobial peptides, cytokines, macrophages, and secretory IgA.

Normal Biota of the Respiratory Tract
Commensal Microorganisms and Microbial Antagonism
The upper respiratory tract harbors a diverse community of commensal microorganisms, which play a protective role by competing with pathogens for resources and space. Even the lungs have a limited normal biota.
Common normal biota: Streptococcus pyogenes, Haemophilus influenzae, Streptococcus pneumoniae, Neisseria meningitidis, Staphylococcus aureus, and Candida albicans.
Microbial antagonism: Normal biota reduce the chances of pathogen colonization.
Variation: The composition of the lung microbiome differs in patients with chronic diseases and between smokers and nonsmokers.
Upper Respiratory Tract Diseases Caused by Microbes
Pharyngitis
Pharyngitis is an inflammation of the throat, often resulting in pain, redness, and swelling. Bacterial pharyngitis tends to be more severe than viral forms and is more likely to be accompanied by fever, headache, and nausea.
Common causative agents: Viruses (as in the common cold), Streptococcus pyogenes (Group A Streptococcus), and Fusobacterium necrophorum.
Symptoms: Pain, inflammation, reddened/swollen mucosa, and sometimes white patches or exudate.

Streptococcus pyogenes: Characteristics and Pathogenesis
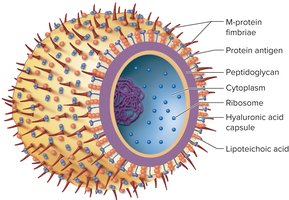
Streptococcus pyogenes is a gram-positive coccus that grows in chains and is a major cause of bacterial pharyngitis. It possesses several virulence factors that enhance its ability to cause disease.
Key features: Nonmotile, forms capsules and slime layers, facultative anaerobe, does not produce catalase.
Pathogenesis: Can lead to complications such as scarlet fever (erythrogenic toxin, sandpaper-like rash, high fever) and rheumatic fever (immunologic cross-reaction with heart tissue).
Virulence Factors of Streptococcus pyogenes
The virulence of S. pyogenes is due to its ability to evade the immune system and produce toxins.
Surface antigens: Mimic host proteins, aiding immune evasion.
Superantigens: Trigger excessive immune responses.
Specialized polysaccharides: Protect against lysozyme.
Lipoteichoic acid: Aids adherence to epithelial cells.
M protein: Resists phagocytosis and enhances adherence.
Hyaluronic acid capsule: Contributes to adhesiveness and immune evasion.
Extracellular Toxins
Streptolysins (O and S): Cause beta-hemolysis and tissue injury.
Erythrogenic toxin: Responsible for the red rash in scarlet fever; produced only by lysogenic strains.
Transmission, Diagnosis, and Treatment of Streptococcal Pharyngitis
Transmission: Respiratory droplets or direct contact with mucus secretions; humans are the only significant reservoir.
Diagnosis: Rapid antigen detection tests and culture on sheep blood agar (beta-hemolysis). Bacitracin disc test helps distinguish from other streptococci.
Treatment: Penicillin is the drug of choice; cephalexin for penicillin-allergic patients. Antibiotic treatment is important to prevent complications.

Other Upper Respiratory Tract Infections
The Common Cold
The common cold is caused by over 200 different viruses, most commonly rhinoviruses. Symptoms include sneezing, scratchy throat, and runny nose. Transmission occurs via indirect contact and droplets.
Sinusitis
Sinusitis can be caused by viruses, bacteria, or fungi, as well as noninfectious factors like allergies. Treatment depends on the cause: antibiotics for bacterial infections, antifungals or surgery for fungal cases.
Lower Respiratory Tract Diseases Caused by Microbes
Pneumonia
Pneumonia is an inflammatory condition where fluid fills the alveoli. It can be caused by bacteria, viruses, or fungi, and is a leading cause of death in children under five worldwide.
Key pathogens: Streptococcus pneumoniae, Legionella pneumophila, Mycoplasma pneumoniae, Chlamydophila pneumoniae, Histoplasma capsulatum, and various respiratory viruses.
Community-acquired vs. healthcare-associated: Community-acquired pneumonia is contracted outside hospitals; healthcare-associated pneumonia is often linked to mechanical ventilation and has higher mortality.
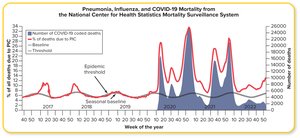
Influenza
Virology and Pathogenesis
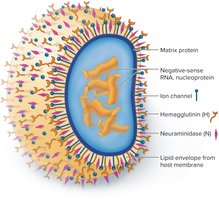
Influenza viruses (A, B, and C) are enveloped RNA viruses with high genetic variability. They cause seasonal epidemics and occasional pandemics.
Key structures: Hemagglutinin (H) and neuraminidase (N) glycoprotein spikes, ion channels, and a segmented RNA genome.
Antigenic drift: Gradual mutation of H and N antigens, requiring annual vaccine updates.
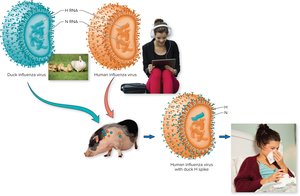
Antigenic shift: Reassortment of RNA segments between different influenza viruses, potentially leading to pandemics.
Transmission, Diagnosis, and Prevention
Transmission: Inhalation of aerosols/droplets, indirect contact with fomites; facilitated by crowding and dry air.
Diagnosis: RT-PCR is the preferred method.
Prevention: Annual vaccination (inactivated or live attenuated); high-dose vaccine recommended for older adults.
Treatment
Antivirals: Zanamivir (Relenza), oseltamivir (Tamiflu), and baloxavir (Xofluza) are effective if administered early.
Tuberculosis
Overview and Pathogenesis
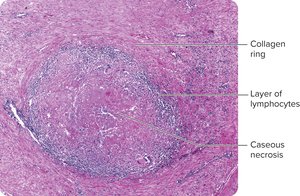
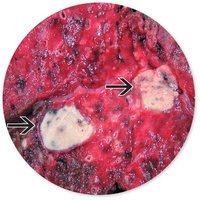
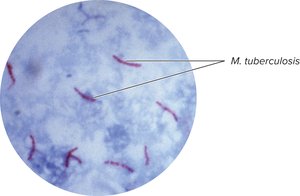
Tuberculosis (TB) is a chronic infectious disease caused by Mycobacterium tuberculosis. It primarily affects the lungs but can disseminate to other organs.
Primary TB: Bacteria multiply in macrophages, leading to tubercle formation and caseous necrosis.
Secondary TB: Reactivation of dormant bacteria causes severe symptoms and lung damage.
Extrapulmonary TB: Infection spreads to lymph nodes, kidneys, bones, genital tract, or brain, often fatal in immunosuppressed patients.
Diagnosis, Prevention, and Treatment
Diagnosis: Tuberculin skin test (Mantoux), interferon-gamma release assays, gene amplification, and acid-fast staining.
Prevention: Limiting exposure, patient isolation, and BCG vaccination (not used in the US).
Treatment: Long-term antibiotic regimens (rifampin, isoniazid); noncompliance leads to multidrug-resistant TB (MDR-TB) and extensively drug-resistant TB (XDR-TB).
Summary Table: Major Infectious Diseases of the Respiratory System
Disease | Main Pathogen(s) | Transmission | Key Features |
|---|---|---|---|
Pharyngitis | Streptococcus pyogenes, viruses | Droplets, direct contact | Sore throat, fever, risk of complications |
Pneumonia | Streptococcus pneumoniae, viruses, fungi | Droplets, aspiration | Alveolar inflammation, high mortality in children |
Influenza | Influenza A, B, C viruses | Droplets, fomites | Seasonal epidemics, antigenic drift/shift |
Tuberculosis | Mycobacterium tuberculosis | Airborne droplets | Chronic, can be latent or active, drug resistance |

