 Back
BackInfectious Diseases of the Genitourinary System: Microbiology and Clinical Implications
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Genitourinary Tract: Structure and Defenses
Overview of the Genitourinary System
The genitourinary tract consists of two distinct organ systems: the urinary tract and the genital (reproductive) system. Both systems are closely linked anatomically and functionally, and are subject to unique microbial threats and defenses.
Urinary tract: Removes metabolic wastes, regulates body processes, forms urine, and transports it out of the body.
Genital system: Primarily functions in reproduction, with distinct male and female anatomical features.
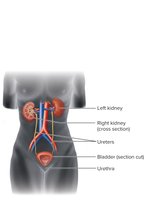
Urinary Tract Anatomy and Defenses
Kidneys: Filter blood and remove metabolic wastes.
Ureters: Tubes transporting urine from kidneys to bladder.
Bladder: Stores urine before excretion.
Urethra: Conduit for urine to exit the body; in males, also part of the reproductive tract.
Defenses of the urinary tract:
Flushing action of urine removes microbes.
Desquamation (shedding) of epithelial cells helps eliminate attached microbes.
Urine contains antimicrobial substances: acidic pH, lysozyme, lactoferrin, and secretory IgA.
Normal Biota of the Genitourinary Tract
The lower urethra harbors a diverse microbiota; upper urinary tract is less colonized.
Female urethra is short and close to the anus, increasing UTI risk.
Penile flora includes Pseudomonas and Staphylococcus species; uncircumcised males have more anaerobes.
Female vaginal biota changes with age and hormonal status; Lactobacillus predominates during reproductive years, maintaining acidic pH.
Urinary Tract Infections (UTIs)
Types and Symptoms
UTIs are common infections of the urinary tract, often caused by normal biota from the gastrointestinal tract.
Cystitis: Infection of the bladder; symptoms include pain, frequent urination, dysuria (burning), cloudy urine, hematuria (blood in urine), low-grade fever, and nausea.
Pyelonephritis: Infection of the kidneys; symptoms include back pain and high fever, with risk of permanent kidney damage.
Urethritis: Infection limited to the urethra.
Causative Agents and Epidemiology
95% of UTIs are caused by GI tract biota; Escherichia coli is responsible for 80% of cases.
Other agents: Staphylococcus saprophyticus, Klebsiella pneumoniae, Proteus mirabilis.
Community-acquired UTIs are more common in women due to anatomical factors.
Catheter-associated UTIs (CA-UTIs) are a significant concern in healthcare settings.
Treatment and Prevention
Nitrofurantoin is commonly used; phenazopyridine relieves symptoms.
Many E. coli strains are resistant to penicillins.
Prevention includes minimizing catheter use and proper hygiene.
Reproductive Tract Infections and Sexually Transmitted Infections (STIs)
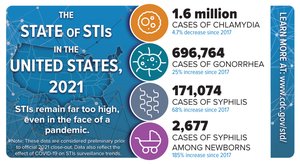
Overview and Epidemiology
Many reproductive tract diseases are sexually transmitted. The CDC reports rising rates of chlamydia, gonorrhea, and syphilis in the U.S.
Discharge Diseases
Characterized by increased fluid discharge from the reproductive tract.
Major examples: Gonorrhea and Chlamydia.
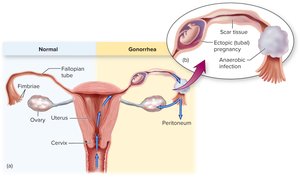
Gonorrhea
Causative agent: Neisseria gonorrhoeae, a Gram-negative diplococcus.
Symptoms in males: Urethritis, painful urination, yellowish discharge; can lead to infertility if untreated.
Symptoms in females: Mucopurulent or bloody discharge, painful urination, risk of pelvic inflammatory disease (PID), infertility, and ectopic pregnancy.
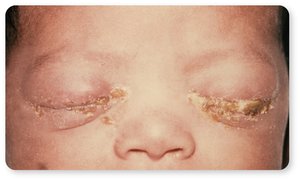
Complications: Dissemination to joints, skin, meninges, or heart; neonatal eye infections (ophthalmia neonatorum).
Virulence factors: Fimbriae for attachment, antigenic variation, IgA protease, endotoxin release.
Diagnosis: Culture, catalase/oxidase tests, carbohydrate fermentation, NAATs.
Treatment: Dual therapy for gonorrhea and chlamydia due to frequent coinfection; antibiotic resistance is a growing concern.
Chlamydia
Causative agent: Chlamydia trachomatis, an obligate intracellular Gram-negative bacterium.
Symptoms: Often asymptomatic; males may have urethritis, discharge, and epididymitis; females may have cervicitis, discharge, salpingitis, and PID.
Complications: Lymphogranuloma venereum, neonatal conjunctivitis, and pneumonia.

Virulence: Intracellular growth, inhibition of phagolysosome fusion, inflammation-induced tissue damage.
Diagnosis: PCR, ELISA, NAATs, urine tests.
Treatment: Doxycycline or azithromycin; treat all sexual partners; rescreen after 3–4 months.
Vaginitis and Vaginosis
Candida albicans (Yeast Infection)
Characteristics: Dimorphic fungus, part of normal biota, can overgrow after disruption of normal flora.
Symptoms: Vaginal itching, burning, discharge; presence of pseudohyphae indicates active infection.

Risk factors: Antibiotic use, diabetes, pregnancy, immunosuppression.
Treatment: Topical or oral azoles; recurrent infections require medical evaluation.
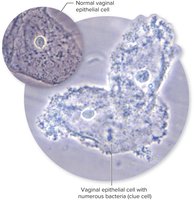
Gardnerella Species (Bacterial Vaginosis)
Symptoms: Fishy-smelling vaginal discharge, little or no inflammation.
Diagnosis: Presence of clue cells (vaginal epithelial cells covered with bacteria) on microscopy.
Treatment: Oral or topical metronidazole or clindamycin.
Trichomonas vaginalis
Protozoan parasite causing vaginitis, often asymptomatic but can cause frothy discharge in females.
Complications: Increased susceptibility to other infections, infertility, adverse pregnancy outcomes.
Genital Ulcer Diseases
Syphilis
Causative agent: Treponema pallidum, a spirochete.
Stages: Primary (chancre), secondary (rash, systemic symptoms), tertiary (gummas, cardiovascular and neurological damage).

Congenital syphilis: Transmitted from mother to fetus, causing developmental defects, stillbirth, or characteristic signs (e.g., Hutchinson's teeth).

Diagnosis: Dark-field microscopy, serology (RPR, treponemal tests), NAATs.
Treatment: Penicillin G is the drug of choice.
Genital Herpes
Causative agents: Herpes simplex virus type 1 (HSV-1) and type 2 (HSV-2).
Symptoms: Painful vesicular lesions, recurrent outbreaks, possible asymptomatic shedding.
Complications: Neonatal herpes (potentially fatal), encephalitis.
Treatment: Antivirals (acyclovir and derivatives) reduce symptoms and recurrences but do not cure the infection.
Summary Tables: Infectious Diseases of the Genitourinary System
Disease | Causative Agent | Main Symptoms | Key Complications | Treatment |
|---|---|---|---|---|
UTI (Cystitis, Pyelonephritis) | E. coli, S. saprophyticus, others | Pain, dysuria, frequent urination, fever | Kidney damage (pyelonephritis) | Nitrofurantoin, symptom relief |
Gonorrhea | Neisseria gonorrhoeae | Discharge, pain, PID, infertility | Neonatal eye infection, systemic spread | Dual antibiotic therapy |
Chlamydia | Chlamydia trachomatis | Often asymptomatic, discharge, PID | Infertility, neonatal conjunctivitis | Doxycycline, azithromycin |
Syphilis | Treponema pallidum | Chancre, rash, gummas | Congenital defects, cardiovascular/neurological damage | Penicillin G |
Genital Herpes | HSV-1, HSV-2 | Painful vesicles, recurrences | Neonatal herpes, encephalitis | Acyclovir, derivatives |
Vaginitis (Candida) | Candida albicans | Itching, burning, discharge | Recurrent infections | Azole antifungals |
Vaginosis (Gardnerella) | Gardnerella spp. | Fishy discharge, clue cells | PID, low birth weight | Metronidazole, clindamycin |
Key Takeaways
The genitourinary tract is protected by physical, chemical, and immunological defenses, but is susceptible to a range of infectious diseases.
UTIs and STIs are common, with significant public health implications due to complications such as infertility, neonatal infections, and chronic disease.
Prevention strategies include barrier protection, screening, prompt treatment, and public health interventions.
