 Back
BackThe Urinary System: Structure, Function, and Clinical Relevance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Urinary System
Overview
The urinary system is essential for maintaining homeostasis by regulating fluid and electrolyte balance, removing metabolic wastes, and controlling blood pressure. The kidneys are the primary organs of this system, supported by the ureters, urinary bladder, and urethra.
Kidneys: Location and Structure
Location of the Kidneys
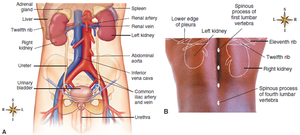
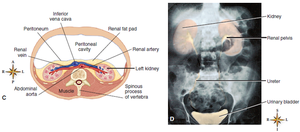
The kidneys are retroperitoneal organs, lying under the back muscles and behind the parietal peritoneum, just above the waistline.
The right kidney is typically positioned slightly lower than the left due to the presence of the liver.
Gross Structure of the Kidney
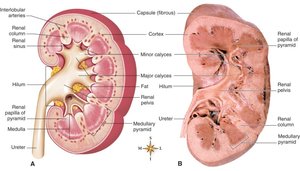
Renal cortex: The outer layer of the kidney, containing the majority of nephrons.
Renal medulla: The inner region, organized into renal pyramids.
Renal pyramids: Triangular divisions within the medulla.
Renal columns: Extensions of cortical tissue between the pyramids.
Renal papilla: The tip of each pyramid, projecting into a minor calyx.
Renal pelvis: Funnel-shaped structure that collects urine and channels it into the ureter.
Renal calyces: Chambers that collect urine from the papillae and drain into the renal pelvis.
Microscopic Structure: The Nephron
Nephron Structure and Types
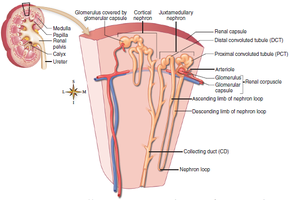
Each kidney contains over one million nephrons, the functional units responsible for urine formation. Nephrons are composed of a renal corpuscle and a renal tubule.
Cortical nephrons: Located primarily in the cortex; comprise about 85% of all nephrons.
Juxtamedullary nephrons: Located near the cortex-medulla junction; play a key role in concentrating urine.
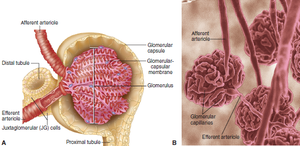
Renal Corpuscle
Bowman capsule (Glomerular capsule): Cup-shaped structure that surrounds the glomerulus.
Glomerulus: A tuft of capillaries where filtration of blood occurs. The afferent arteriole brings blood in, and the efferent arteriole carries it away, creating high pressure for filtration.
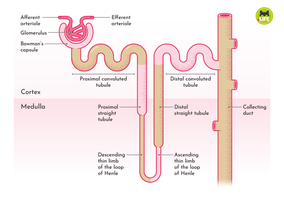
Renal Tubule
Proximal convoluted tubule (PCT): First segment after the Bowman capsule; major site of reabsorption.
Henle loop (Nephron loop): U-shaped segment with descending and ascending limbs; crucial for concentrating urine.
Distal convoluted tubule (DCT): Segment after the ascending limb; involved in selective secretion and reabsorption.
Collecting duct (CD): Receives urine from multiple nephrons and channels it to the renal pelvis.
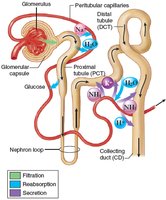
Renal Physiology: Formation of Urine
Filtration
Filtration is the first step in urine formation, occurring in the renal corpuscle. Blood pressure forces water and solutes from the glomerulus into the Bowman capsule, forming filtrate.
Normal glomerular filtration rate (GFR): 125 mL/min (about 180 L/day).
Reabsorption
Reabsorption is the process by which water, ions, and nutrients are reclaimed from the filtrate back into the blood, primarily in the PCT, loop of Henle, DCT, and collecting duct.
About two-thirds of filtered water is reabsorbed in the PCT by osmosis.
Sodium reabsorption in the nephron loop uses a countercurrent mechanism, creating a hypertonic medulla to concentrate urine.
Chloride ions follow sodium passively due to electrical attraction.

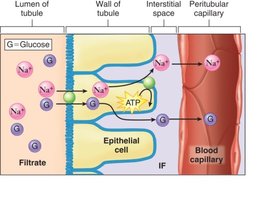
Reabsorption of Glucose
Glucose is reabsorbed in the PCT via sodium-glucose co-transporters.
The transport maximum is the highest amount that can be reabsorbed; excess glucose appears in urine (glycosuria), as seen in diabetes mellitus.
Renal threshold: The plasma concentration at which glucose begins to appear in urine.
Secretion
Secretion is the final step, involving the active transport of substances such as hydrogen ions, potassium ions, urea, uric acid, creatinine, and certain drugs from the blood into the distal tubule and collecting duct.
Ammonia is secreted by diffusion.
Some diuretics increase potassium secretion, leading to 'potassium-wasting.'
Hormonal Control of Urine Volume
Key Hormones
Antidiuretic hormone (ADH): Promotes water reabsorption in the collecting ducts, reducing urine volume.
Aldosterone: Increases sodium and water reabsorption, reducing urine volume; part of the renin-angiotensin-aldosterone system (RAAS).
Atrial natriuretic hormone (ANH): Increases sodium and water excretion, increasing urine volume.
Atypical Urine Volumes
Anuria: Absence of urine production.
Oliguria: Scanty urine output.
Polyuria: Excessive urine output.
Urinary Tract Anatomy
Ureters
Narrow tubes lined with mucous membrane and muscle, draining urine from the renal pelvis to the bladder.
Urinary Bladder
Elastic, muscular organ lined with mucosa arranged in rugae for expansion.
Stores urine prior to voiding.
Urethra
Narrow tube leading from the bladder to the exterior.
Serves as a passage for urine (and semen in males).
Common mucous membrane lining allows infections to spread throughout the urinary tract.
Micturition (Urination)
Process and Control
Regulated by internal (involuntary) and external (voluntary) urethral sphincters.
Emptying reflex is triggered by bladder wall stretch, leading to contraction and sphincter relaxation.
Control Problems
Incontinence: Involuntary urination; types include urge, stress, overflow, reflex, and neurogenic bladder.
Retention: Urine is produced but not voided.
Suppression: No urine is produced.
Urinalysis
Purpose and Methods
Physical, chemical, and microscopic examination of urine.
Assesses color, turbidity, odor, specific gravity, pH, urea, proteins, glucose, and presence of abnormal substances.
Microscopic analysis can reveal casts, cells, and crystals indicative of pathology.
Renal and Urinary Disorders
Obstructive Conditions
Hydronephrosis: Swelling of the renal pelvis and calyces due to urine flow obstruction.
Renal calculi (kidney stones): Crystallized minerals that may block urine flow and cause severe pain (renal colic).
Tumors: Renal cell carcinoma and bladder cancer, often presenting with hematuria.
Urinary Tract Infections (UTIs)
Commonly caused by gram-negative bacteria.
Urethritis: Inflammation of the urethra.
Cystitis: Inflammation of the bladder.
Pyelonephritis: Inflammation of the renal pelvis and kidney connective tissue.
Glomerular Disorders
Damage to the glomerular-capsular membrane can cause proteinuria, hypoalbuminemia, and edema.
Acute glomerulonephritis: Often follows streptococcal infection; immune-mediated.
Chronic glomerulonephritis: Progressive, immune-mediated damage leading to renal failure.
Kidney Failure
Acute renal failure: Sudden, often reversible loss of kidney function.
Chronic renal failure: Gradual, irreversible loss of nephrons due to chronic disease.
Polycystic kidney disease (PKD): Hereditary disorder with multiple cysts destroying kidney tissue.
Progression of Kidney Failure
Stage 1: Compensation by healthy nephrons.
Stage 2 (Renal insufficiency): Loss of function leads to uremia (high blood urea nitrogen, BUN).
Stage 3 (Uremic syndrome): Complete failure; requires dialysis or transplantation for survival.
Additional info: The urinary system's role in homeostasis is closely linked to nutrition, as it regulates the excretion of metabolic waste products from protein and other nutrient metabolism, and maintains electrolyte and fluid balance essential for cellular function.
