 Back
BackWater and Minerals: Essential Roles in Human Nutrition
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Water and Minerals in Human Nutrition
Introduction
Water and minerals are fundamental nutrients required for the maintenance of health and physiological function. This chapter explores their roles, requirements, sources, and the consequences of imbalances, providing a comprehensive overview for nutrition students.
Water
Functions of Water
Water is vital for life, serving multiple physiological roles:
Transport: Transports nutrients and oxygen to cells.
Solvent: Acts as a solvent for vitamins, minerals, glucose, and amino acids.
Metabolic Reactions: Participates in metabolic reactions.
Waste Elimination: Facilitates the elimination of waste products.
Lubrication: Is a major component of mucus and other lubricating fluids.

Water Balance
Water balance refers to the dynamic equilibrium between water intake and output. Under normal conditions, these are approximately equal (ex. not sick). The sensation of thirst and the hormone vasopressin regulate daily fluid balance.
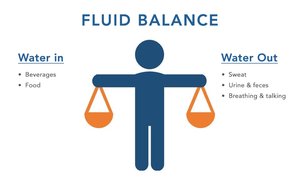
Water Output
Sensible Losses: Measurable losses from urine and feces. (measurable)
Insensible Losses: Immeasurable losses from respiration (breathing) and skin. (immeasurable)
Average Loss: Adults lose approximately 1750–3000 mL of water daily. loses 1-3 L
1,000 ml = 1 Liter (1L)
Factors Increasing Loss: Extreme temperatures, exercise, high altitude, and low humidity.
Water Intake
Sources: Liquids, solid foods, and metabolic water.
Average Intake: About 2.5 L/day (80% from fluids, 20% from food, 250–350 mL from metabolism).
Water Recommendations
Fluid intake is adequate when urine is pale yellow.
Dark urine is dehydrated
Men aged 19 and older for AI is 3.7L/day
Older adults and children should not delay drinking until thirsty.
8oz = 240ml of water
Estimating Body Fluid Requirements
Body fluid requirements vary based on age, activity, environment, and health status. Monitoring urine color and frequency can help assess hydration status.
30ml/kg for the average adult
30ml = 1 ounce
30ml/kg x 70kg = 2100ml/day
Ex. Pt weight = 55mg. 30ml x 55kg = 1,650 ml = 1.65 L
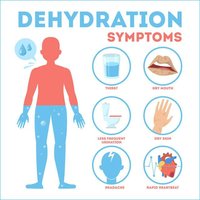
Dehydration
Dehydration results from inadequate fluid intake and is characterized by:
Impaired mental function and motor control
Increased body temperature during exercise
Increased resting heart rate
Increased risk of heat stroke
Hypovolemia (Deficit of Body Fluids)
A net water loss of 1–2% of body weight causes thirst, fatigue, and weakness; 7–10% loss leads to severe symptoms and can be fatal if untreated. Clinical situations increasing water loss include vomiting, diarrhea, and hemorrhage.
Fluid and Electrolyte Balance
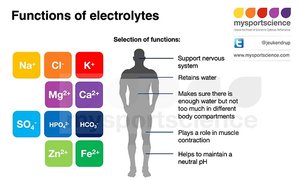
Electrolyte Distribution and Function
Body fluids are regulated by membranes, electrolyte concentration, and hydrostatic pressure. Electrolytes are ions that help regulate nerve and muscle function, acid–base balance, and water balance.
Cations: Positively charged ions (e.g., sodium Na+, potassium K+).
Anions: Negatively charged ions (e.g., chloride Cl-).
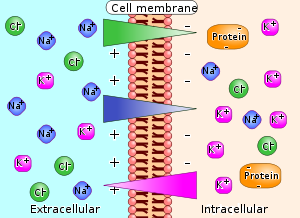
Electrolyte Movement and Osmosis
Electrolytes attract water, and their concentration determines fluid movement between compartments via osmosis. Sodium and chloride are predominant in extracellular fluid, while potassium and phosphate are major in intracellular fluid.
Electrolyte Balance and Regulation
The kidneys maintain electrolyte concentrations through filtration and excretion. Imbalances can result from dehydration, overhydration, medications, or organ disorders.
Feedback mechanism

Minerals
Major vs. Trace Minerals
Minerals are classified based on the amount present in the body:
Major Minerals: Present in amounts >5 g (e.g., calcium, phosphorus, magnesium, sulfur, sodium, potassium, chloride).
Trace Minerals: Present in smaller amounts (e.g., iron, iodine, zinc, selenium, copper, manganese, fluoride, chromium, molybdenum).
Mineral Balance and Toxicity
Maintained by storage, absorption, and excretion adjustments.
Toxicity can result from excessive supplementation or environmental exposure. (not seen commonly)
Mineral interactions affect absorption and function; total diet must be considered.
Sources of Minerals
Unrefined foods are richer in minerals than refined foods.
Supplements can contribute but food sources are preferred.

Major Electrolytes
Sodium (Na+)
Major extracellular electrolyte; 98% absorbed from diet.
Homeostasis maintained by urinary excretion and hormones (aldosterone).
AI: 1500 mg/day (age 14+); recommended <2300 mg/day.
Excess intake is common and associated with hypertension risk.

Potassium (K+)
Major intracellular electrolyte; essential for muscle and heart function.
*Normal range: 3.5–5.0 mEq/L.
Dietary sources: bananas, apricots, spinach, broccoli, potatoes.
Imbalances (hyperkalemia (above 5.0)/hypokalemia(below 3.5)) can cause heart dysrhythmias.
Nutrient dense diet
Chloride (Cl-)
Works with sodium to maintain fluid balance and osmotic pressure.
Major Minerals
Calcium (Ca)
Most abundant mineral; 99% in bones and teeth.
Bone serves as a reservoir for blood calcium regulation.
Balance maintained by vitamin D and parathormone (PTH).
Dietary sources: milk, yogurt, cheese, kale, broccoli, sardines, salmon.
Hypocalcemia: muscle spasms; Hypercalcemia: constipation, kidney stones, muscle weakness.

Calcium and Phosphorus Relationship
Calcium and phosphorus have an inverse relationship in the body; as one increases, the other decreases.

Magnesium (Mg)
Deficiency is rare due to renal conservation.
Function: protein synthesis
Food: Nuts, Seeds
Excess: trouble breathing
Defiency: Seizures
Risk factors: type 2 diabetes, celiac disease, GI surgery, alcohol abuse, aging, certain medications.
Sulfur (S)
Component of amino acids (methionine, cysteine), biotin, and thiamin.
Important for protein structure in skin, hair, and nails.
Food: Chicken, Turkey, Cabbage, Diary products
Excess: Brain fog, increased risk of heart disease
Deficiency is rare except in severe protein deficiency
Trace Minerals
Iron (Fe)- Will be on test
Two-thirds found in hemoglobin; also in myoglobin, enzymes, and storage proteins (ferritin).
Heme iron (animal sources) is more bioavailable than nonheme iron (plant sources).
RDA: 8 mg (men, postmenopausal women), 18 mg (premenopausal women).
Food: Dark chocolate, meat
Excess;
Deficiency leads to iron deficiency anemia (IDA): fatigue, weakness, pallor, dizziness.
Vitamin C enhances absorption; dairy inhibits absorption.
When diagnosed with anemia (Ferrous Sulfate is given)
Fe is better absorbed with Vitamin C (orange juice), Diary decreases absorption of Fe
Causes poop to be dark tarry stool, constipation
Increase fiber and water
Fe taken orally (through straw or beyond teeth) when touching teeth it damages

Zinc (Zn)
Essential for wound healing, immune function, cell division, and growth.
Sources: nuts, oysters, red meat, poultry, beans.
Excess: nausea, vomiting, increase prostate cancer for men
Deficiency risk: poor intake, alcoholism, malabsorption, vegetarianism, sickle cell disease

Iodine
Component of thyroid hormones (T3, T4). regulate temperature
Sources: seaweed, iodized salt, seafood, dairy, eggs.
Excess:
Deficiency can cause hypothyroidism and goiter.
Hypothyroidism occurs when intake falls below 10-20mcg/day (goiter)

Other Trace Minerals
Selenium
Nuts, seafood, cereals, diary products
Defiency:
Copper
RBC production
Nuts, seeds, whole grains
Nausea, stomach pain
Anemia - deficiency
Manganese
Excess:
Fluoride: Promotes tooth enamel mineralization and reduces dental caries.
Chromium: Enhances insulin action and glucose regulation.
Water and Minerals in Health Promotion
Optimal health is promoted by choosing healthy beverages, reducing sodium intake, and ensuring adequate intake of potassium and calcium. Adopting a healthy eating pattern supports mineral balance and overall well-being.
